



Learning Disability Interventions: Making Sense of The Evidence
Introduction
Effective individualized treatment is the prescription for any child diagnosed with a learning disability (LD). However, choosing the right treatment can be a daunting and confusing process. Controversies with respect to the efficacy of many LD interventions abound. How does an “intervention consumer” make sense of the vast array of treatments that are available? As with any potential purchase it is always wise to investigate before buying. To be an informed LD treatment consumer means evaluating the scientific validity of a treatment before accepting claims of efficacy.
The importance of being an informed LD intervention consumer
Frustrated parents of children with untreated LD are especially vulnerable to empty promises of miracle cures and treatment breakthroughs. Desperate for solutions, some may impulsively choose controversial untested treatments. Uninformed choices not only waste time, energy and possibly finances but can potentially subject already overburdened children to unnecessary frustration and failure. Although there will always be uncertainties associated with any treatment, carefully weighed choices will reduce the risk of wasted resources, disappointment and learning setbacks.
The efficacy of available LD treatments
Swanson points out that we are biased by the publication of only positive outcomes in intervention research (Swanson, 2000). This practice leads to the impression that all treatments work and are equally effective. Unfortunately the fact that an LD intervention is available to the public does not mean that it has been proven or even tested. As well, popularity and even widespread use are not valid indicators of efficacy. In the absence of any formal regulations monitoring the value of available LD treatments, even unsubstantiated treatments can be openly promoted and sold to the public.
Understanding claims of proof
Consumers should not be expected to intuitively grasp the notion of scientific proof. The requirements for the designation “evidence-based” are far more involved and stringent than is generally assumed. Further, the procedures and criteria of the scientific method, which forms the basis of proof, are simply not common knowledge. To recognize this is the first step toward learning to distinguish valid from unfounded LD treatments.
It is not surprising that false or misleading claims about LD treatments are regularly and successfully marketed to the general public. Those who make invalid allegations depend on consumers’ lack of research expertise for their success. The less consumers understand about scientific validity, the easier it is to sell unsubstantiated treatments as proven interventions. Unless consumers make deliberate efforts to become informed they will be ill equipped to judge the validity of LD interventions and have no basis with which to make sound treatment choices.
To legitimately promote a treatment as effective requires proof. If there is no mention of testing, research, or evidence, it is highly unlikely that the intervention in question has been subjected to any kind of scientific inquiry. Without research support, allegations of treatment validity remain unsubstantiated and should be viewed with caution and even skepticism. This is not to say that interventions without an evidence-base are necessarily ineffective. It simply means that claims of treatment efficacy should be reserved for interventions that have been subjected to proper scientific investigation. Unfortunately, this is often not the case with treatment promotions regularly being made in the absence of proof.
Beware of subjective reports
Testimonials, anecdotes and personal accounts although sometimes compelling do not constitute scientific evidence. Even if accurate, subjective reports are based on individual cases that do not generalize to other situations. Stories of treatment success are of value if they provide hope and direct consumers to investigate new interventions but they do not qualify as proof and should never be thought of as such.
How to determine if an intervention has research support
The terms “research”, “evidence”, “support” tend to be used loosely and sometimes haphazardly. In reality there is good research and bad research. More often than not research does not meet the standards of proper scientific investigation. Alleged evidence might be scientific or anecdotal, systematically determined or casually gathered. Even among valid research studies, only a small percentage provide decisive information about treatment efficacy.
The first step in evaluating any claim of research support is to locate the source of the alleged evidence. By whom, when, and how was the information obtained? If there truly is evidence supporting the effectiveness of an intervention, it should be made available to the consumer. More often than not, simply locating the source of the research (or finding that it does not exist) will be enough to determine whether or not claims of support are justified. If there is systematic research underlying a claim of proof, reference will be made to a particular study or studies. Research published in academic journals will be identified by a reference which lists the author(s), date, article title, journal title, volume, and page number of the research study.
The publication of research in a peer reviewed journal is one indication of its quality and means that the research has been reviewed and scrutinized by a panel of experts in the field. While publication in a peer reviewed journal does not guarantee scientific rigor, an absence of peer reviewed research is a very good indication that any allegations of proof are false.
Not all research findings qualify as proof
Unfortunately, the majority of published intervention studies lack scientific rigor. In a comprehensive synthesis of 30 years of learning disabilities intervention research, Swanson and colleagues examined evidence from 900 different LD intervention studies. Of these 900 studies, only 25% met the author’s criteria for inclusion in the analysis. Further, of the 25% included in the synthesis, only 5% met the high standards of proper research methodology (Swanson, et al., 1999). The results of this review highlight the complexities of scientific research and the difficulties associated with establishing proof.
Clearly, treatments should not be regarded as valid simply because published studies have been cited. Second-hand accounts of research findings are only interpretations of actual results and are frequently biased, misleading or altogether incorrect. In the process of interpretation, results can be inadvertently or intentionally misrepresented. In order to determine the actual outcomes of an intervention study it is advisable to consult the original source of the cited research whenever possible.
The original research source, although more accurate and reliable than secondary interpretations, is often more difficult to understand. All experimental studies use some form of statistical analysis which can be incomprehensible to non-experts. Indeed researchers themselves spend years studying and learning about the statistical analysis of data. It is not recommended or at all necessary to become an expert in statistical analysis to understand claims of intervention efficacy. A review of the introduction and discussion sections of the research report will be sufficient to get a general sense of any significant findings and their interpretation by the authors. Because the research has been subjected to peer review, definitive claims of treatment efficacy will only be made if they are justified by the results.
The scientific method
Investigators use several kinds of research to further our understanding of LD interventions. Three common designs include descriptive analyses, large-scale field studies, and experimental designs. All of these approaches contribute to our understanding of LD interventions but not all can provide us with proof of treatment efficacy. Evidence for treatment validity can only be obtained through the use of experimental designs which follow the scientific method.
When intervention research adheres to the standards of the scientific method, valid claims of efficacy can be made with a minimum of bias. Using the scientific method, researchers first form a hypothesis or idea which is then formulated as a prediction (e.g. “treatment X will help children with LD learn to read”). An experiment is then designed to test this prediction. The nature of the treatment, how it will be implemented, and the means for evaluating treatment efficacy are all objectively defined and described in detail prior to conducting the intervention. Pre and post intervention measures are obtained with the use of objective measures.
The most credible intervention studies always control for alternative explanations of the research findings. A control group is composed of individuals who are similar to participants in the treatment group on most important measures such as age, type of disability, etc. However, the control group does not receive the treatment. Without a comparison control group there would be no way of knowing whether the treatment or some other factor caused observed changes in behavior or performance.
Once an experiment has been conducted, statistical tests are carried out to determine if any treatment effects are scientifically meaningful or simply due to chance. If statistically significant results are found, the research must then be subjected to scrutiny by experts in the field before being accepted for publication in peer reviewed academic journals. Finally, for a finding to be considered well established, the research must be confirmed through replication by independent researchers in the field.
Successful research does not equal successful implementation
Once a particular intervention is shown to be effective through properly controlled experimentation, the process of implementation can begin. Implementation involves transferring what has been established in a controlled research setting to the everyday environment. The conditions of carefully controlled experimentation can be quite different from real life circumstances. The very things that are controlled for during intervention studies form a critical part of real life and cannot be ignored during treatment implementation. Challenges associated with transferring research findings to the real world make the process of implementation perhaps as daunting as the process of proving treatment validity.
Conclusions
Obtaining scientific proof of LD treatment efficacy, replicating valid findings, and finally implementing proven interventions is an extremely lengthy, arduous and costly process. This fact coupled with the intense demand for effective LD treatments has led to the proliferation of a myriad of unsubstantiated LD interventions.
To be an informed LD intervention consumer means learning to distinguish evidence-based treatments from unsubstantiated claims of treatment efficacy. Fortunately, there are clearly defined steps that can be taken to verify any allegations of proof. The general recommendation for the LD intervention consumer is to proceed with caution, become informed, and scrutinize any claims of efficacy. An awareness of the complexities of intervention research will perhaps encourage LD consumers to have patience when making important decisions regarding LD treatments.
References
Hoagwood, K., Burns, B.J., Kiser, L., Ringeisen, H. & Schoenwald S.K. (2001). Evidence-based practice in child and adolescent mental health services. Psychiatric Services, 52(9), 1179-1189.
Swanson, H. L., Hoskyn M., & Lee, C. M. (1999). Interventions for students with learning disabilities: A meta-analysis of treatment outcomes. New York: Guilford Press.
Swanson, H.L. (2000). Issues facing the field of learning disabilities. Learning Disability Quarterly, 23, 37-50.
Reprinted with permission from Community Health Systems Resource Group
Hospital for Sick Children. April 15th, 2002
Copyright © 2002 The Hospital for Sick Children, All rights reserved. You are free to duplicate this document but we request that you acknowledge The Hospital for Sick Children copyright.
![]()
Learning Disabilities Statistics
Some recent Canadian sources for statistics on learning disabilities
Preamble
In the field of Learning Disabilities (LDs), statistics on incidence rates can be particularly vulnerable to distortion or bias for a number of reasons. For example, there is no precise operational definition of learning disabilities that is widely accepted, with the result that studies are inconsistent in how they define what they are measuring. Similarly, studies vary in how they treat the disorder known as ADD/ADHD. Some include this as a specific type of LD involving attention, memory and concentration, others partial it out a separate but related and often co-existing disorder, while still others don’t mention it at all. Many incidence surveys are based on self-reporting, so their results depend on what the respondents understand about LDs, and also whether they are comfortable with disclosing. All these factors may help explain why estimates of the incidence rate of LDs range from as low as 2% of the population to as high as 10% or more.
There are other examples of potential biases and distortions in the way data can be interpreted. Therefore any statistical analysis should be interpreted with caution and only with a full understanding of the definitions and criteria used by the researchers.
Ministry of Education (EDU) statistics
- In the 2015-16 academic year; approximately 40% (39.8%) of students, identified as “exceptional” by an Identification, Placement and Review Committee (IPRC) in Ontario, were identified under the Communications/Learning Disability category and definition.
- The total percentage of students identified as exceptional was 8.8% of the school population. That would mean that 3.5% of the school population was identified for special education under Learning Disability in 2015-16.
- This figure does not take into account the large number of students who receive special education programs and services without being formally identified. In total, 17.3% of students in Ontario received some special education programs and/or services in 2015-16. If approximately the same percentage of these students had learning disabilities, then about 6.9% of students in Ontario publicly funded schools in 2015-16 would have learning disabilities (identified or unidentified).
Ministry of Training, Colleges and Universities (MTCU) statistics
Statistics from MTCU (from Colleges and Universities Year End Reports):
- College students with learning disabilities (excluding those in Apprenticeship programs) rose each year from 8,007 in 2008-09 to 10,971 in 2014-15. However, students with LDs comprised a decreasing percentage of the total number of students with disabilities served by the offices for students with disabilities (DSOs), from 33% in 2008-09 to 25% in 2014-15.
- University students with learning disabilities rose each year from 5,620 in 2008-09 to 7,064 in 2014-15. This number as a percentage of total number of students with disabilities served by DSOs declined from 42% in 2008-2009 to 36% in 2014-15.
The good news is that more students with learning disabilities are attending colleges and universities in Ontario. The concerning news is that there are more students with a range of disabilities who are served by offices for students with disabilities, and funding may not keep up to the increasing demand on these offices.
Transitions Longitudinal Study 2009
This study, begun in 2005, surveyed a cohort of students (initially about 200) who had participated in pilot transitions support programs from 1998 -2002 in one of the 13 colleges and universities in Ontario under the Learning Opportunities Task Force (LOTF). The longitudinal study shows that students with learning disabilities who got supports in postsecondary studies and answered the surveys had more favourable outcomes than those shown in the PALS research. For example:
- For each of the five years of the study, 10% or less of the participants left their programs without graduating, compared to 15% in the general population. For those who did not graduate, the most common reason was inability to pass required courses.
- The number of participants who returned to school after graduation each year ranged from 17% to 35%.
- The number of participants who were employed increased from 58% in 2005 to 82% in 2009.
- By 2009, 93% of participants who responded to the survey earned at least $20,000 and 53% earned at least $35,000.
- About half of the employed participants had disclosed their LDs at work and of these 96% found the reaction positive. 43% of employed participants did not feel that disclosure was necessary.
Canadian Survey on Disability, 2012: Learning disabilities among Canadians aged 15 years and older
In this survey, adults (15 and older) with a learning disability were identified as those who answered the question “Do you think you have a condition that makes it difficult in general for you to learn? This may include learning disabilities such as dyslexia, hyperactivity, attention problems, as well as other conditions” or “Has a teacher, doctor or other health care professional ever said that you have a learning disability?”
NOTE: Because it is based on self-reporting, the population surveyed may have included some with intellectual disabilities.
- The prevalence of learning disabilities ranged by age from 2.0 % to 3.1 % of the population, with an average of 2.3%.
- Learning disability rates among men and women were not significantly different.
- 96.3% of respondents who reported a learning disability also reported at least one other type of disability.
Education
- Among the respondents who were currently not attending school, 33% had not completed high school but 35.6% had completed postsecondary education.
- Among those who currently were in school or had recently been in school, almost all (98%) stated that their disability directly impacted their educational experience (The most common impacts were taking longer to achieve education milestones, changing their choice of courses or career, and taking fewer courses. Many also reported social difficulties, including being avoided or excluded, and being bullied).
- 51.4 % of respondents who recently attended school required some sort of ‘education aid or service’. Of these, 93.9% stated that at least some of their needs had been met, while 6.1% felt that none of their needs had been met.
- About 32.8% stated they needed at least one type of learning aid, such as computers with voice recognition, and of these 41.2% reported this need was not met, usually because the cost was too high.
Employment
- 39.2 % of respondents in the 25 to 34 age group and 37.2 % in the 35 to 44 age group were employed.
- Among those who were or recently had been employed, 55.5% stated they needed at least one type of work accommodation. Of these, 71.0% stated at least some of their needs had been met while on the job.
- Among those with employment income, median employment incomes for adults with a learning disability were less than half for those without any disability ($15,900 and $34,100 respectively).
Canadian Survey on Disability, 2012: Persons with disabilities and employment
NOTE: These statistics are not specifically for individuals with LDs.
- Among university graduates, the employment rate of those with a moderate disability (adjusted for age differences) was 77%, compared with 78% among those with a mild disability and 83% among those without a disability (Chart 2). The difference between university graduates with a mild or moderate disability and those without a disability was not significant.
- Conversely, the lack of a high school diploma may represent more of a barrier among those with disabilities. Among people who had not completed high school, 33% of those with a moderate disability were employed, compared with 50% of those with a mild disability and 65% of those without a disability.
- Only 40.6 % of children with LLs had all their needs for assistive technologies met, while 31.2 % had no needs met. Computers were the most common assistive device, and cost was the biggest factor in unmet needs.
www.statcan.gc.ca/bsolc/olc-cel/olc-cel?catno=89-628-XWE&lang=eng
Participation and Activity Limitation Survey (PALS), 2006
PALS is a Canadian national survey designed to collect information on adults and children who have a disability, whose everyday activities are limited because of a condition or health problem. It is based on self-reporting.
www.statcan.gc.ca/pub/75-006-x/2014001/article/14115-eng.htm
Learning limitations were defined as: Difficulty learning due to the presence of a condition, such as attention problems, hyperactivity or dyslexia, whether or not the condition was diagnosed by a teacher, doctor or other health professional.
Children (5 to 14)
- Among children aged 5 to 14, learning limitations (LLs) was the largest disability reported (about 69.3% of the children with disabilities).
- LLs affected 121,080 of the children aged 5 to 14, which is 3.2% of all children in this age group.
- Of children 5 to 14 in the survey who required special education, 89.6% did so because of LLs.
- 51.4% of parents who had children with LLs reported difficulty obtaining special education.
Putting a Face on Learning Disabilities (PACFOLD), LDA of Canada 2007 Report (www.pacfold.ca)
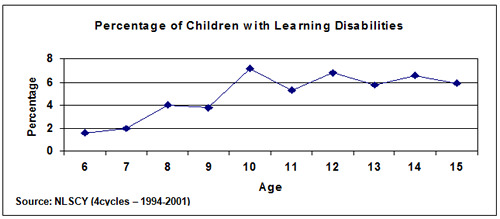
The National Longitudinal Survey of Children and Youth (NLSCY) began following a representative sample of Canadian children from birth to 11 years in 1994, with follow-up surveys conducted every two years.
PACFOLD summarized data for Ontario from the NLSCY, from 1994 to 2001:
- 2% of children aged 6 to 15 were reported by parents/guardians to have a learning disability
- 5% of parents of children with learning disabilities (LDs) said their child was doing well or very well at school, compared to 76.1% of parents of children without disabilities.
- 16% of children with LDs received help or tutoring outside of school, compared to 5% of children without disabilities
- 7% of parents of children with LDs said that their child had been diagnosed with emotional, psychological or nervous difficulties, while parents of children without disabilities reported only1% of such diagnoses
PACFOLD reported that 4.9% of Canadian children aged 6 to 15 had a learning disability according to the NLSCY. However, this figure varied across the age spectrum, from a low of 1.6% for children aged 6, to a high of 7.2% for 10-year-olds.
Other PACFOLD results:
- A significant number of youth and adults with LD had dropped out of the education system altogether, with over one-quarter of Canadians aged 22 to 29 with LD reporting less than a high school certificate as their highest academic achievement
- Persons with LDs were 2 to 3 times more likely to report fair to poor physical, general, and mental health, and 2 to 3 times less likely to report very good to excellent physical, general and mental health than the general population
- Persons with LDs were more than twice as likely to report high levels of distress, depression, anxiety disorders, suicidal thoughts, visits to a mental health professional and poorer overall mental health compared to persons without disabilities
SUMMARY OF LD Statistics
- Estimates of the incidence rate of LDs range as high as 10% or more of the population, but there is most statistical evidence from demographic sources for a range of 4 to 6 %.
- Figures from the Ministry of Education suggest that about 6% of students in the publically funded school system are receiving special education programs or services because of learning disabilities.
- The numbers of postsecondary students with LDs in both colleges and universities is increasing steadily, but their percentage of the caseloads of offices for students with disabilities is decreasing.
- Outcomes are promising for students with LDs who get the supports they need to reach postsecondary education and who receive supports in postsecondary.
- Employment rates for those who complete university is not significantly different from other students.
Learning Disabilities Association of Ontario
Tel: (416) 929-4311
Web: www.LDAO.ca
Document first created in February 2009, updated in February 2018
Author: Peter Chaban
Source: Reprinted with permission from the author
Amongst identified exceptional students in Ontario, pupils with behavioural/emotional disorders represent 6 percent of the exceptional population and 0.53 percent of the overall school population*. As with learning disabilities, the definition used for this exceptionality has been controversial. Unlike, learning disabilities which defines its expcetionality within the context of a neurological etiology, behavioural disorders can occur as a result of neurological, psychological and environmental factors. As a result, the behavioural definition has to capture a diverse student population. At present, the definition for behavioural/emotional disorders includes the following criteria:
- The student’s behaviour deviates in a significant manner from that expected for the situation.
- The behaviour breaks from age, social and cultural norms.
- Inappropriate behavior is consistently exhibited in at least two different settings.
- The behaviour may be compulsive and/or impulsive, sad or withdrawn.
- The behaviour may represent poor interpersonal relationships
Students who are identified as behavioral/emotional may have their behaviour described as internalizing or externalizing behaviour. Although this description gives a quick snapshot of the student’s behaviour, it does not allow for a clearer understanding of all the factors maintaining the behaviour. One such factor is a learning disability.
The relationship between learning disabilities and behaviour/emotional problems is complex. One area of interest to researchers has been the association between learning disabilities and psychopathology. In one study by Cantwell and Baker(1991), 600 children were identified as speech/language impaired and 300 of these children were followed up 5 years later. Of these children, 25 percent had learning disabilities and 75 percent of the LD children had a psychiatric illness. The most prominent diagnosis fell under the spectrum of anxiety disorders and a minority were diagnosed with depression. Other studies have pointed out that though LD children are not likely to suffer from depression more often than those in the general population, children who have both learning disabilities and depression reported less self-esteem, were more detached and had a bleaker view, than depressed children without learning disabilities.
Another area of interest is the relationship between learning disabilities and somatic complaints. Margalit and Raviv (1984) compared the prevalence of somatic complaints in learning disabled children with two control groups. In the LD group, 54 percent had somatic complaints as opposed to 9 percent and 13 percent in the two control groups. The primary complaint amongst the LD group was fatigue.
A third area where learning disabilities and behavioral problems coexist is with social behaviour. Often children with learning disabilities have problems with familial and peer relationships. This may be the result of processing problems which make it difficult for LD children to pick up social cues. This in turn may result in avoidance behaviour. This type of behaviour is often used as a defense to avoid stress generated by social interactions. Children who are unable to develop avoidance defenses may use irritable or aggressive behaviour to cope with stress associated with social interactions.
When learning disabilities and behavioural problems appear together, it is important to identify whether the behaviour is secondary to the learning disability or co-morbid. When the negative behaviour is caused by the learning disability, the solution to that behaviour often lies in dealing with the learning disability. When it is co-morbid, the interventions become more complicated, since the behaviour has to be treated separately from the learning disability. In this case, the burden of suffering should be seen as the primary problem. If it is the behaviour presenting the greatest suffering, then it should be managed first and if it is the learning disability, then it will become the top priority. Often when dealing with the complexity of coexisting learning disability and behavioural problems, finding the solution becomes a process of trial and error. Whatever the situation, it is important to be aware of the distress caused when the complex interactions of learning, emotions and behaviour are hampered by a learning disorder.
References:
Cantwell, D.P. & Baker, L. (1991) Association Between Attention Deficit-Hyperactivity Disorder and Learning Disabilities. Journal of Learning Disabilities, Vol. 24(2), 88-95
Margalit, M. & Raviv, A. (1984) LD’s Expressions of Anxiety in Terms of Minor Somatic Complaints. Journal of Learning Disabilities. Vol. 7(4), 226-228
*from Statistical Services Section, Policy Analysis and Research Branch, Ministry of Education for 1990-91.
Author: LDAO staff
Source: Learning Disabilities Association of Ontario, 2000
The most common disorder that co-exists with learning disabilities is attention deficit/hyperactivity disorder (ADHD). Many studies over the years have indicated a very strong co-morbidity of the two conditions but the exact percentage of overlap varies widely in these studies because of methodological inconsistencies. Studies of the families of children with either learning disabilities or ADHD indicate strong patterns of inheritance for both conditions, but also show that they are independent disorders.
ADHD and learning disabilities are two discrete disorders with distinct symptom clusters. However, some symptoms may be common to both disorders, including: disorganization, weak executive functioning, and inefficient use of strategies. Without careful assessment, distinguishing between ADHD and learning disabilities can be difficult because of overlapping symptoms and because some behaviours that may result from learning disabilities can look like ADHD symptoms. For example, individuals with central auditory processing deficits can appear inattentive, and students who have become discouraged due to learning problems may not stay on task or may appear distractible.
Assessments for ADHD and learning disabilities follow a different process, although both can be addressed in a multidisciplinary assessment. Psychoeducational testing by a registered psychologist or designated psychological associate is required to diagnose learning disabilities. Assessment for ADHD is usually through a clinical interview and review of developmental history, with the use of standard checklists and some cognitive tests being common.Diagnosis of ADHD is done by a pediatrician, psychiatrist or psychologist.
It is important to distinguish between the two conditions because of different methods of treatment. Intervention for learning disabilities may involve academic skills instruction, the development of compensatory strategies and self-advocacy skills, and appropriate accommodations. Treatment for ADHD may include behavioural strategies, modifications to the learning environment, family counselling, and the use of specific medications such as Ritalin.
To conclude, ADHD is not considered a learning disability. A learning disability is a neurologically based disorder affecting the psychological processes necessary for learning. ADHD is an associated disorder that can interfere with the individual’s availability for learning. Assessment and treatment methods are different for the two conditions.
Author: LDAO
Source: LDAO
Individual Education Plans
Every student in the publicly-funded school system who receives special education services must have an Individual Education Program (IEP). The IEP process creates an opportunity for teachers, parents, school administrators, related services personnel, and students (when appropriate) to work together to increase the chances of academic success. To create an effective IEP, parents, teachers, and often the student, must come together to look closely at the learner’s unique needs and design an educational program to help the student succeed.
According to the Ontario Ministry of Education, an IEP is “a written plan describing the special education program and/or services required by a particular student, based on a thorough assessment of the student’s strengths and needs.”
It is important to distinguish what an IEP is not. The document is not a description of everything that will be taught to a student, a daily lesson plan or a document that records all learning expectations.
IEPs may be prepared without an Identification Placement and Review Committee (IPRC), but the written decision of the IPRC is the only guarantee that a student will be entitled to services he or she requires.
Once the IPRC has made its statement of decision, the principal is notified and becomes responsible for ensuring the IEP is prepared and implemented.
Information gathering for the IEP should include a review of the student’s records (e.g. IPRC statements of decision and recommendations), relevant assessment data, consultations with school personnel and other professionals, and any information gained through observation of the student.
Consultations with parents and students are an important part of the process.
The Ministry recommends a collaborative team approach, where information on a student’s strengths and needs can be shared, and plans can be made on teaching strategies, accommodations, technology supports, and assessment techniques.
Parents and students should be part of the IEP team. Parents and students (16 and over) must be consulted on the development of the IEP, and sign a form to affirm they were consulted in the development process.
The principal must see that the IEP is complete, that copies are sent to the parents and student (if 16 or older), and that all relevant school personnel are aware of the IEP’s content. The principal is responsible for ensuring that the IEP is implemented. However, parents also need to check that all teachers are aware of and understand the contents of the IEP. Parents and students should collaborate with teachers to make sure the provisions are implemented. If students themselves understand and accept the IEP provisions, this can go a long way toward successful implementation.
The IEP must be reviewed and learning expectations updated at least once in every reporting period (i.e. each term where there is a report card). According to The IEP Resource Guide (2004), “If certain strategies cease to be effective, it is imperative that the staff working with the student seek out and implement new teaching methods and accommodations”. Once again, parents and students are to be consulted if there are significant changes to the student’s learning expectations or accommodations.
In 2000 the Ministry of Education issued standards for Development, Program Planning and Implementation of IEPs. Between 2001 and 2003, the Ministry conducted reviews of IEPs prepared by school boards across Ontario. On the basis of information gathered through these reviews, and consultations with educators and parents, a revised IEP Resource Guide was published in 2004. The complete guide can be found at:
www.edu.gov.on.ca/eng/general/elemsec/speced/guide/resource/index.html
Improving Executive Function Skills
An Innovative Strategy that May Enhance Learning for All Children
Janie did well in school until she got to fourth grade. Then her grades dropped, she couldn’t keep up with her work load, she got frustrated, and her self-esteem was sinking. Janie was referred for testing for special education, but she scored well on the assessments. What was wrong? Janie’s difficulties in school stemmed from executive function (EF) weaknesses. Janie is not alone. While children who have learning disabilities, autism, ADHD, traumatic brain injury, and conduct disorder often have difficulties with EF, more children without disabilities are exhibiting EF problems as well.
While definitions vary, EF generally refers to the cognitive processes that enable individuals to engage in goal-directed or problem-solving behaviors. Thus, EF may include goal setting or identifying a problem, developing a plan, the ability to execute the plan, flexibility, attention and memory systems to guide the individual (e.g., working memory), and evaluation or self-monitoring.
Some are now recommending that all children be taught EF processes systematically starting in the elementary grades. One reason is that even in early elementary grades teachers are requiring students to complete long-term projects, as well as lengthy reading and writing assignments—all of which require EF, says Lynn Meltzer, co-founder and co-director of the Institute for Learning and Development and professor at Tufts University. A second reason is that in today’s technologically reliant society, students often turn to the Internet or other technology for information.
“We live in an Internet-driven society,” says Meltzer. “Students are not taught from information that is pre-organized by experts…it is critical that every child is taught these kinds of strategies. They impact all aspects of student work as they move up in grade levels. Students must coordinate multiple subskills in second grade.”
While all students benefit from instruction in EF strategies, such instruction is even more critical for students with disabilities. Research has shown that students with cognitive disabilities and behavior disorders often have weaknesses in EF. With explicit instruction, these students may develop the EF skills, which can help them progress academically and socially.
How Effective Is EF Training?
At this point, research on EF training is still limited. Torkel Klingberg, a neuroscientist at the Karolinska Institute in Sweden, and his colleagues conducted a study of children with ADHD. They found that better working memory skills may reduce ADHD symptoms. In another study, children trained in the EF skill of selective attention were quicker to respond than the control group. These results suggest that EF training may affect the way children’s brains develop. However, there is much to learn in this area. For example, the brain’s adaptations in response to EF training may be gradual and accumulative, and training may be needed for an extended period of time. Also, EF training would need to continue to challenge children’s skills.
What Happens When EF Is Weak?
Difficulties in EF have long-ranging consequences. Some obvious effects of EF impairment includes children’s ability to organize materials, plan long-term projects, manage time, and persist in accomplishing an academic goal such as a term paper or reading a long book. EF weakness also makes it difficult for students to start and complete tasks, and their ability to handle frustration is compromised.
EF problems also manifest themselves in academic tasks such as reading or writing an essay, state Meltzer and Kalyani Krishnan in Executive Function in Education: From Theory to Practice. Some of the EF processes involved in reading include 1) drawing on prior knowledge as students shift from “retrieving and interpreting background knowledge to attending to and interpreting print and new content,” 2) flexibility as students interpret words, draw inferences, and process redundant information, and 3) prioritizing as students decide which parts of the text is useful for their purpose. Writing requires students to plan, engage in flexible thinking (paraphrasing the topic), organize, and prioritize.
Students with EF problems may also be poor test-takers. First, they are unable to prioritize which information to study when preparing for the test. As they take the test, they are unable to prioritize tasks, plan responses, or monitor their time.
EF problems can also manifest themselves through behavior problems. Failure to plan, to inhibit behavior despite intentions, and to evaluate can all lead students to act inappropriately, according to Philip David Zelazo, professor at the University of Toronto, in his AboutKidsHealth series on EF. For example, some children may act inappropriately, because they do not plan or anticipate the consequences of their behavior. In other instances, children who cannot inhibit their actions may continue to behave inappropriately even when they understand the consequences of those actions; children who have difficulty evaluating may not be able learn from punishment and will therefore repeat inappropriate behavior.
EF and Disabilities
Specific EF impairments appear to affect particular disabilities. Children with learning disabilities have difficulty with numerous facets of EF, according to Meltzer and Krishnan. These include self-regulatory activities such as checking, monitoring, and revising when learning as well as weaknesses in cognitive flexibility, sorting, organizing, and prioritizing information.
“Their (students with learning disabilities) strong conceptual reasoning abilities may not match their output and productivity because of their difficulties organizing and prioritizing numerous details, juggling these details in working memory, and shifting flexibly between abstract concepts and literal details as well as from major themes to the details,” state Meltzer and Krishnan in Executive Function in Education.
Some researchers see ADHD not just as a problem of paying attention but as a weakness of EF, says Thomas E. Brown, professor at Yale University, in “ADHD as Executive Function Impairments” in the Help Group Newsletter. Hyperactivity or impulsivity could stem from a student’s inability to control his or her actions or verbalization, both of which can be manifestations of EF problems, he says. Children with ADHD may also manifest EF impairments that impact organizing, planning, and remembering.
“The core of their problem (individuals with ADHD) is a developmental impairment in being able to manage their mind to focus on tasks they need to do, even when those tasks are not immediately interesting,” Brown says in the article.
Meltzer says students with learning disabilities and ADHD share a similar EF problem—information overload.
“These students have information coming into a funnel that needs to be processed and prioritized,” she says. “They also have to figure out what is most important, ignore the irrelevant information, and shift from the main idea to details. They can’t. The funnel is clogged, and as a result these students can’t produce the kind of projects and essays required.”
Children with autism, too, show deficits in EF. Specifically, these individuals have difficulty in planning future actions and cognitive flexibility.
Assessing EF
Assessing EF, especially in children, is a complex task. Just of couple of factors that can skew results are that individuals’ results on EF assessments may vary due to their anxiety level or they may perform well on tasks in an assessment setting but not when faced with similar tasks in the real world, especially when novelty is a feature of the situation. Also, it is difficult to parse out one area that is the source of EF difficulty.
That said, some of the assessments used to determine EF ability include:
- Stroop Color Word Task—Measures an individual’s ability to inhibit responses, resolve interference, and resolve behavioral conflict.
- Go–No Go Task—Measures an individual’s attention, flexibility of responding, and ability to withhold a response.
- Stop-Signal Task—Measures an individual’s ability to stop a response that is already underway.
- Tower of Hanoi—Measures an individual’s ability to plan ahead.
- Wisconsin Card Sorting Test—Measures an individual’s ability to test hypothesis and flexibility.
Strategies to Strengthen EF
Though EF strategies can—and often are—taught in one-on-one settings or in small groups, some recommend that all students be taught EF strategies in general education classes.
“We need to teach executive function strategies so students can plan, organize, prioritize and use their working memory effectively,” says Meltzer. “Then students become efficient and successful; their self-esteem improves and their effort becomes more goal-oriented. All students benefit from the strategies, and some students must have them. If we embed the strategies in the curriculum, all students benefit.”
A few models of classroom-based EF strategy instruction are available, including the Kansas intervention model, Benchmark model, and Drive to Thrive, according to Meltzer in her book, Executive Function in Education. All of these models share common principles:
- Strategy instruction should be directly linked to the curriculum.
- The strategies should be taught explicitly, including teacher modeling and extensive practice.
- Strategies should be taught in a structured, systematic way.
- Strategy instruction should address students’ motivation and effort.
One way to implement the above is for educators to teach a strategy a week, says Meltzer.
As a follow up, create a “Strategy of the Week Board,” on which students post their favorite strategy. This also creates a springboard for a discussion of the strategies.
However, EF strategies are not a “one size fits all.” For students to use EF strategies effectively, as a first step they must understand their own learning profile and their strengths and weaknesses as well as which strategies work for them, according to Meltzer.
“You need to teach the strategies for the school and classroom, as well as for the individual child,” she says. “Then you help students become metacognitive learners who can understand how they learn.”
Examples of EF Strategies
Special educators already use many of the strategies that help students improve EF, such as checklists and “how to” lists, breaking long assignments into chunks, and using visual calendars, time organizers, and mnemonics.
Meltzer takes these strategies a step further. Some examples from Executive Function in Education are:
- Memorization—When using acronyms to help students memorize information, the “crazier the phrase,” the better. If a student is non-verbal, then make a cartoon.
- Cognitive Flexibility—To help students improve cognitive flexibility, work with riddles and jokes to help students shift between word meanings. In math, students can ask themselves: do I know another way to solve this problem, does this look similar to other problems I have seen, is this problem the same or different from the one before it?
- Prioritizing—To help students prioritize information, teach students to listen to the teacher’s intonation during lectures. Also, students can highlight the most important ideas in a text in one color and details in another color.
- Notetaking—To help students prioritize and remember information students can take 3-column notes: the first column contains one word that is the core concept, the second column contains the details supporting the concept, the third column contains the strategy the student will use to remember the information. When taking notes from text, students can use a 2-column approach. In the first column, students ask themselves questions about the text, and they put the answers in the second column.
- Self-Monitoring and Self-Checking—Helping students check their work requires two processes: 1) Provide explicit checklists for assignments, so students know what to check for, and 2) Help students develop personalized checklists, so they become aware of and check for their most common errors. As a final step, students can make their own acronyms to remind themselves of their personal error traps.
Resources
Executive Function in Education: From Theory to Practice, editor, Lynn Meltzer
National Center for Learning Disabilities, http://www.ncld.org/content/view/865/391/
Center for Research on Learning, Strategies Intervention Model, http://www.specialconnections.ku.edu/cgi-bin/cgiwrap/specconn/searchabledb/moreinfo.php?desc_id=154
Tools of the Mind, http://www.devcogneuro.com/research.html#ongoing
Language, Speech and Hearing Services in Schools, Vol. 30, 265-274, “What Are Executive Functions and Self-Regulation and What Do They Have to Do with Language-Learning Disorders?”, http://www.architectsforlearning.com/sitebuildercontent/sitebuilderfiles/singerbashir1999.pdf
Author: Henri Audet, Executive Director, Camp Kirk
Undoubtedly, this is one of the questions most often asked by parents as their child reaches the age where a camping experience becomes an option. I might add that “option” is the operative word and here is why. There are many different programs and recreational experiences available for children today, and certainly camp is one of them, but camp is not necessarily the be all and end all. So, my first recommendation would be that parents thoroughly research all of the options available to them for their child before making a final decision. Having said this, I might point out that, particularly for children with learning disabilities and those with ADD or ADHD, where socialization and low self-esteem is a concern, a camping experience may offer just the right recipe to help a child learn the skills necessary for him or her to become the best that they can be. No, camp is not a cure, but it can certainly set a child on the path to success and as parents or educators, what more can we ask for?
The other important point I would like to make is, to include your child as early as possible in the process, no matter which options you are looking at. First and foremost, this is meant to benefit the child, notwithstanding the fact that moms, dads and care givers indirectly benefit as well, if you know what I mean… So make it “fun” for everyone.
Once you have made the decision that camp is the desired option, then here is what you do. First, you contact the Ontario Camping Association at 416-781-0525 and ask for their camping guide which lists all of the camps accredited by the Association. Basically what the OCA accreditation process does, is give its member camps the “Good Housekeeping Seal of Approval.” In other words, every accredited camp has met the required standards of the Association, thereby assuring prospective campers and their families of a minimum standard of quality in every aspect of a camp’s operation.
While you are waiting to receive the directory, you and your child need to spend time to answer some very basic questions, e.g., What do we want from camp? What length of time best suits our needs? Is an all girls, all boys or co-ed setting best for our child? What type of program and/or philosophy are we looking for? Are there special physical, emotional or mental needs we should consider or compare to the camp’s ability to meet them?
After you have received the OCA directory, you might want to do a preliminary read through and, based on your child’s and your own priorities and expectations, simply go through an initial process of elimination. A checklist for choosing a camp might include the following: health and safety procedures, emergency procedures, name of director, quality of living space, quality of dining area and of food preparation, quality and balance of camp program, staff training and experience, general supervision and camper/staff ratio, ability to meet special needs, references from other parents, and accreditation from OCA or similar associations.
Once you have made a short list of potential camps, then call the director of each camp and request a camper application package. Upon receipt of this material, sit down with your child, read each camp brochure, and keeping in mind your priorities and your child’s needs, evaluate the camps, make notes and check marks, particularly around things which come across in the brochure as being outstanding. The reason for this is that you want to make sure that what you saw or read is really what happens at this camp. Even though camp brochures are designed primarily as a selling tool, they can provide you with invaluable information about the camp. Do read between the lines, however. For example, if a camp puts a great deal of emphasis on its past history, perhaps it has failed to evolve and keep up with the changing times, both in terms of program and recreational and/or educational philosophy.
One of the most important steps in choosing a camp is to have an opportunity to meet the camp director, or at least a representative, in person, either at an open house, or preferably in your home. You will want to ask about his or her background in camping, about the camp’s philosophy and about the camp’s provisions for campers with special needs. This is your chance to ask any questions or to raise any concerns you or your child might have about the camp or the program. One crucial point here is that parents and/or guardians of a child, particularly one with special needs, must be completely up front as to their child’s condition, his/her specific requirements and their expectations. You will find that, under most circumstances, camp directors are more than willing to make the necessary adjustments to meet a child’s needs. This face to face meeting is also the camp director’s opportunity to start forming a relationship among himself, a prospective camper and his/her family. Remember, your child’s camping experience may span several years, so the relationship you develop with each other may prove to be very significant. Therefore, if a director is unable or unwilling to facilitate this, as a parent I would be concerned.
Let me end simply by stating that, regardless of your own past camping experiences, or what other people may have told you, in my opinion and based on my experience of over 20 years in the camping business, no camp can and should claim to be suitable for every child. Moreover, no responsible camp director will ever give you a guarantee that your child will succeed at camp. Even though it is understood that every parent wants to make absolutely sure that they are doing the best for their child, one must also understand that there are simply too many variables to be able to guarantee a successful camping experience. The real and only issue here is that all children, regardless of their abilities or disabilities, should be given a choice based on their individual needs and their own goals and aspirations, as they relate to a camp’s philosophy, resources and capabilities. It is up to everyone concerned to make sure that the best possible choices are made, and that ultimately, the child is the “winner.”
Author: Gary Direnfeld, MSW
With all the attention on where your kids are going, little may have been said about where they are leaving. Each year thousands of children leave home and some for the very first time.
Parents would do well to remember their first experience of leaving home. For many it came easily, but for some it was accompanied by stress and for others conflict. In remembering their own experience, parents next have to consider the experience they want to provide their son or daughter.
This experience of leaving home is important psychologically for children, now young adults, and parents alike. The experience can set the tone for the next stage of family development; adult-to-adult relationship with your child. Remember, they will likely be married some day and you will want to see your grandchildren.
So no more telling a child what to do. After managing through adolescence, parents are faced with the fact that their child is a young adult. Long gone are the days of parental authority. Coming to terms with this fact lies at the heart of the leaving home experience and can impact on your son or daughters sense of adult security and your future relationship together.
Perhaps it is not so much that the parents must reassure their children that they will be all right, but that the parents must reassure themselves and not let their concerns impede the children’s departure. Let them leave in peace and do not try to cram in all the lessons left untaught. Some lessons are only gained by leaving home.
For a better leaving home experience consider these suggestions:
- Talk with your son or daughter about their feelings of leaving home. Don’t push on whether they will miss you though, as this feeling might actually be your own. If it doesn’t come up, then maybe the thought hasn’t crossed their mind in the excitement of the experience.
- Reminisce with them about their growing up and the pleasures you have had along the way. Marvel at their growth and accomplishments and your anticipation of future accomplishments.
- Plan well for the departure so the actual moment isn’t fraught with last minute errands or conflicts. Offer your help and be prepared to stand back or jump in – only as requested or discussed. Your hand is no longer attached to the bicycle seat and you have to let go now again.
If you follow these suggestions you may experience a smoother transition to an adult relationship with your son or daughter. This kind of experience can repair past conflicts with your child and improve the odds of having a great relationship as adults.
Gary Direnfeld is a social worker, child-behaviour expert, and author of Raising Kids Without Raising Cane (Secrets of the Trade, 1992). His presentations provide insights on issues ranging from child behaviour management and development; to family life; to socially responsible business development. Courts in Ontario consider Gary an expert on matters pertaining to child development, custody and access and social work.
Author: Tamarah Kagan-Kushnir, MD, FRCPC, and Jay Rosenfield, MD, MEd, FRCPC
As pediatricians our ultimate goal is to optimize the health and well being of children and facilitate their growth and development. Learning disabilities threaten a child’s quality of life in a variety of spheres, including educational achievement and social/emotional development. As such, helping a child and family to recognize and manage a learning disability as early as possible is an important part of comprehensive Pediatric care.
In many ways, pediatricians are in a unique position to be able to identify developmental risk factors which might be the early precursors of a learning disability. The pediatrician is often the first person parents consult when they have concerns around their child’s development and learning. Furthermore, pediatricians see children over time and therefore have the opportunity to make repeated observations of a child, thus forming a more accurate and complete picture of their development. This, along with parents’, teachers’, and other caregivers’ observations, allows for early recognition of any difficulties. Having knowledge about normal and abnormal development, the pediatrician can then put these concerns in perspective and identify what further measures need to be taken.
As pediatricians are often the first professionals to be aware of a child’s difficulties, they are often responsible for selecting and coordinating a multidisciplinary team to address a child’s needs, including early and accurate diagnosis and intervention. As the medical professional on the team, ruling out medical problems causing or contributing to a child’s developmental picture is a key role. This includes deciding what, if any, medical investigations or procedures are necessary, and whether or not specific treatments, such as medications, are required.
Moreover, a significant number of children with learning disabilities have coexisting problems, including attentional and emotional difficulties such as depression or anxiety, which might benefit from medical intervention. To enhance communication between team members, pediatricians often liase with the other professionals involved in the child’s care. As they see the child regularly, they are also in a position to provide follow up and reassessment of the efficacy of interventions as well as the need for further evaluations and referrals.
Acting as a support and resource to parents is an integral part of what a pediatrician does for all children, especially those with special needs. This includes providing parents with information and helping them to access resources, not only for assessment and therapy, but also for further education and support. Pediatricians can also assist parents in putting together the reports from the variety of professionals interacting with their child so that they can develop a comprehensive understanding of their child’s strengths and weaknesses. Ultimately, parents are a child’s most important advocates. Empowering them to do this effectively and helping them negotiate “the system” is an on-going process between the family and the pediatrician.
Working together, parents and pediatricians can accomplish a great deal in helping the young child maximize his/her potential and future success. Parents will always know their children best, and therefore often recognize difficulties before any professionals do. To benefit from their pediatrician’s expertise and support in this area, it is important for parents to discuss their concerns with their pediatrician. Effective communication is a critical aspect of the care and advocacy for the learning disabled child, and can be a powerful tool in achieving early and accurate diagnosis.
Understanding Dyslexia
Dyslexia is a learning disability involving difficulties with different forms of language. These can include problems with reading, spelling, understanding spoken language and/or expressing oneself in speaking or writing.
Dyslexia, like other learning disabilities, is not related to intelligence. An unexpected gap exists between a person’s academic achievement and their intellectual ability (which may be very high).
People with dyslexia may have talents in many areas, in addition to their areas of difficulty. Each person’s pattern of strengths and weaknesses is unique to them. In other words, no two dyslexics are alike. That is why assessment is very important.
Common Signs of Dyslexia:
Early signs
- difficulty learning to talk
- difficulty listening and following directions
- difficulty remembering
- difficulty pronouncing words correctly or expressing ideas clearly
In school
- difficulty learning the alphabet
- difficulty sequencing letters or numbers
- difficulty rhyming
- difficulty with sequence and memory for words
- difficulty learning to read, write and spell
About Phonological Processing
Extensive studies have shown that children diagnosed with dyslexia consistency differ from other children in an ability called “phonological processing”. Phonological processing involves the ability to notice, think about, and manipulate the individual sounds in words (phonemes).
A phoneme is the smallest sound portion of a word, smaller than a syllable. Children have to be able to hear and distinguish phonemes in words before they can attach letters or letter combinations to them. Rhyming is an early activity encouraging the development of “phoneme” awareness.
Diagnosis & Treatment
Diagnosis of dyslexia is based on a comprehensive assessment that may include tests of: intellectual ability, expressive and receptive language (both oral and written), academic achievement in reading, spelling, vocabulary, comprehension, handwriting and composition. Recommendations for educational remediation should be contained in a written report.
Appropriate remedial programming for dyslexia may include the following:
- direct instruction of language skills and concepts.
- systematic, step-by-step sequential teaching of the alphabetic phonic system of language
- multisensory instruction, involving seeing, listening, touching and doing
Dyslexia is something that people are born with, and in many cases there appears to be a family history. Ongoing research is documenting differences in the structure and organization of the brains of people with dyslexia.
Dyslexia is not outgrown, but with appropriate education, understanding and time, many people with dyslexia learn to read and write, and go on to develop their special abilities and talents. They may be very successful in their chosen careers. A number of well-known scientists, artists, athletes and business and political leaders have dyslexia.
Author: Ruthmary Deuel, M.D., Betty Sheffield, and Diana Hanbury King
Source: Reprinted with permission.
What is dysgraphia?
Dysgraphia means difficulty with handwriting. There are several different kinds of dysgraphia. Some people with dysgraphia have handwriting that is often illegible and shows irregular and inconsistent letter formations. Others write legibly, but very slowly and/or very small. When these individuals revert to printing, as they often do, their writing is often a random mixture of upper and lower case letters. In all cases of dysgraphia, writing requires inordinate amounts of energy, stamina and time.
Dysgraphia can interefere with a student’s ability to express ideas. Expressive writing requires a student to synchronize many mental functions at once: organization, memory, attention, motor skill, and various aspects of language ability. Automatic accurate handwriting is the foundation for this juggling act. In the complexity of remembering where to put the pencil and how to form each letter, a dysgraphic student forgets what he or she meant to express. Dysgraphia can cause low classroom productivity, incomplete homework assignments, and difficulty in focusing attention.
Emotional factors arising from dysgraphia often exacerbate matters. At an early age, these students are asked to forego recess to finish copying material from the board, and are likely to be sent home at the end of the day with a sheaf of unfinished papers to be completed. They are asked to recopy their work but the second attempt is often no better than the first. Because they are often bright and good at reading, their failure to produce acceptable work is blamed on laziness or carelessness. The resulting anger and frustration can prevent their ever reaching their true potential.
What causes dysgraphia?
A few people with dysgraphia lack only the fine-motor coordination to produce legible handwriting, but some may have a physical tremor that intereferes with writing. In most cases, however, several brain systems interact to produce dysgraphia. Some expersts believe that dysgraphia involves a dysfunction in the interaction between the two main brain systems that allows a person to translate mental into written language (phoneme-to-grapheme translation, ie. Sound to symbol, and lexicon-to-grapheme translation, ie. mental to written word). Other studies have shown that split attention, memory load, and familiarity of graphic material affect writing ability. Typically, a person with illegible handwriting has a combination of fine-motor difficulty, inability to revisualize letters, and inability to remember the motor patterns of letter forms.
Who is qualified to diagnose dysgraphia?
Dysgraphia cannot be diagnosed solely by looking at a handwriting sample. A qualified clinician must directly test the individual. Such a test includes writing self-generated sentences and paragraphs and copying age-appropriate text. The examiner assesses not only the finished product, but also the process, including posture, position, pencil grip, fatigue, cramping or tremor of the writing hand, eyedness and handedness, and other factors. The examiner may assess fine-motor speed with finger-tapping and wrist turning.
What is the treatment for dysgraphia?
Prevention, remediation and accommodation are all important elements in the treatment of dysgraphia. Many problems can be prevented by early training. Young children in kindergarten and grade one should learn to form letters correctly; kinesthetic memory is powerful and incorrect habits are very difficult to eradicate.
Muscle training and over-learning good techniques are both critical for the remediation of dysgraphia. Specifically designed exercises are needed to increase strength and dexterity. A specialist can recommend the most appropriate plan of exercises. For all students, kinesthetic writing, that is writing with eyes closed or averted, is a powerful reinforcer. Work needs always to begin with the formation of individual letters written in isolation. Alphabets need to be practiced daily, often for months.
Finally, individuals can benefit from a variety of modifications and accommodations. One effective method is to teach the use of a word processor, bypassing the complex motor demands of handwriting. Many students may find learning the keyboard by the alphabet method easier than beginning with the home keys. For many, touch typing offers a whole new opportunity to learn to spell through a different kinesthetic mode. Students should also experiment with different writing tools; some people with dysgraphia may find pencil grips helpful. Other bypass methods include allowing a student to answer questions orally or into a tape recorder instead of writing, modifying written assignments so that less writing is required, and allowing extended time to complete tests and assignments. Copying from the board is an especially difficult task. Teachers need to provide notes. Photocopying the notes of another student is one possibility. Providing an outline, with spaces left for the student to fill in information, is another. Writing on a slightly inclined plane may be helpful.
Should people with dysgraphia use cursive writing instead of printing?
For many children with dysgraphia, cursive writing has several advantages. It eliminates the necessity of picking up a pencil and deciding where to replace it after each letter. Each letter starts on the line, thus eliminating another potentially confusing decision for the writer. Cursive also has very few reversible letters, a typical source of trouble for people with dysgraphia. It eliminates word-spacing problems and gives words a flow and rhythm that enhances learning. For children who find it difficult to remember the motor patterns of letter forms, starting with cursive eliminates the traumatic transition from manuscript to cursive writing. Writers in cursive also have more opportunity to distinguish b, d, p, and q because the cursive letter formations for writing each of these letters is so different.
Author: By James A. Cincotta, MA Ed
Source: reprinted with permission of the author
Disclosure refers to telling a supervisor, co-worker or others about your learning disability. Disclosure is one of the most difficult decisions you can make. It’s a personal decision that requires a lot of thought and planning. You need to carefully plan how you wish to disclose and think about the possible implications this action has for everyone involved.
Reasons Why Adults with LD Keep It To Themselves.
- May not know much about their LD and how it affects them at work
- Had an unpleasant experience in the past, and do not want to repeat that experience
- Fear that disclosing will lead to prejudice, discrimination or rejection
- May think that a LD will be seen as a weakness
- Feel they should not disclose their LD unless it is absolutely necessary. They prefer to work around the problems.
- Do not know when or how to disclose their LD .
Some Reasons Why you Might Decide to Disclose:
- Because the requirements of your job have changed due to organizational growth, restructuring or technological changes, and you can no longer “hide” your learning disability
- Because clear-cut issues have arisen that allow your supervisor to gain a better understanding of your situation
- Because you want to explain why you have not always met expectations or requirements of the job.
Some Situations When You Might Decide to Disclose
- Before a job interview, or before you accept a job or a promotion so you can discuss the accommodations you require
- During a job evaluation
- When your LD begins to hamper your work performance
- At other times, when you think your employer and/or co-workers are receptive to your disclosure.
When Not to Disclose
- When companies recruit people with LD but lack a supportive environment allowing people with LD to excel.
- When you believe that a person or the company will use the information to prevent your success
- When you feel that people will make you feel bad about your LD
- When you are at a job interview, because there is a risk of not being selected for the job due to your LD or the focus is put on your LD, not your skills
To Whom Do You Disclose?
The best person to talk to is a staff person from the human resources department, or at least removed from the front-line. In small companies, you may want to speak to a senior person who is not your direct supervisor.
Some Helpful Tips About Disclosing
- Plan a meeting. Scheduled meeting between yourself and the person you have decided to talk to.
- Be prepared. Provide the person with a specific reason for the accommodation. Explain why you need it and how this would benefit the organization.
- Don’t discuss your life history. Provide only as much information as the person needs to know for you to obtain the accommodation.
Information discussed should be private. Stress that the information needs to remain confidential and private. Ask if anyone else will be given the information and for what reasons? - Make a plan and stick to it. Write an action plan on how, when and to what extent the accommodation is to be provided.
- Follow up. Request a follow-up meeting to chart the progress or adjustment which needs to be made.
Think It Over, Carefully
- Before you disclose, think carefully about what you are going to say. Remember, it is important to emphasize your strengths and successes, and list any strategies or accommodations that have worked for you in the past.
- Ultimately, only you can decide the time, the place and the amount of information to share with others.
Strategies to help individuals at work
Accommodations on the Job
- Accommodations are the different methods and materials that a person with learning disabilities uses to complete tasks or activities with greater ease and efficiency.
- According to Canadian Human Rights legislation, employees have a right to accommodations in the workplace if it does not cause “undue hardships” to the company or the organization where you work. Undue hardship means the accommodation is not too expensive or too hard for the employer to put in place.
Accommodation Means:
- Making changes to the environment without changing the nature of the task or activities
- The specific equipment used (e.g. computer, tape recorder) to get the job done
- Techniques (extra time, quiet working space, written and verbal instructions) to make communications with supervisors and co-workers flow better
- Matching the tools, techniques or strategies to the specific need.
Auditory: Best Practices
- Assistive Technology (A computer that can read to the individual or help with spelling)
- Reduce background noise (ie. Sitting under a vent could distract a person conversation; make them aware and move elsewhere )
- Repeat instructions
- Have listener repeat back information to you and allow extra time for information processing
- Offer written instructions, charts, pictures, ie. Declaration
- Demonstrate the task first rather than discussing it
You have difficulty remembering what you heard.
- Make sure that verbal instructions are given away from background noises such as ringing telephones, noisy machinery or background conversations.
- Ask to move to a quieter location.
- Ask if you can have a written copy.
- Take notes or ask for written instructions.
Organization: Best Practices
- Use timers or verbal response as reminders
- Map information / graphic organizers
- Allow extra traveling time and time to process
- Allow client to work at own pace
- Break task into component parts or sub-tasks
- Help in mapping out a day or projects.
- PDA’s / Daytime / Alarms
You have difficulty telling time and you arrive late or unusually early.
- Use alarms or bells, etc., to signal changes.
- Schedule extra time for travel between meetings and interviews.
- Use timers or verbal response as reminders.
Have difficulty organizing your work day, tasks, files or paper work
- Use a day planner or agenda book. Regularly keep it up to date. Check it before you leave for work.
- Use colour pens and highlighters to colour code and prioritize tasks and activities. Use “sticky” notes which can be removed once the task is completed.
- Break down larger activities into smaller tasks. Ask for specific timelines and due dates to complete work. Ask which tasks are urgent and which can wait.
- Use time reminders, such as a watch, alarm clock, stop watch or buzzers.
Visual Perception: Best Practices
- Provide a room in neutral colours with minimal physical distractions
- Use oral communication and web-based materials instead of written documentation
- Voice Activated Software
- More time to complete tasks
- Talking Calculator
- Position person so their back is facing the door
Attention: Best Practices
- Always on the move, fidgeting (feet/pencil tapping), you can’t sit still.
- Take frequent exercise or stretch breaks. Be careful not to take too many because you don’t want to let people think you’re not working.
- Keep a soft rubber ball that you can squeeze and play with. Make sure that by playing with the ball you are not bothering anyone.
- Take the time to exercise at home or at a gym before going to work to burn off energy. Consider walking to work.
- Write down the time of day when you fidget the most. When you are the most active, use that time to run errands, talk to people, or do the type of work that allows you to burn off the excess energy.
Have difficulty organizing your work day, tasks, files or paper work (cont.)
- Buy a good, easy-to-use time management book or take classes in time management from a community college or adult high school which will teach you how to better organize your time.
- Use time management software which can schedule your meetings and activities and organize your emails.
- Work in groups or ask a co-worker to help you.
Author: Dr. Glen DiPasquale
Comorbidity is described as a situation where two or more conditions that are diagnostically distinguishable from one another tend to occur together. The exact nature of the relationship between comorbid conditions is a matter of some debate in the research literature (Martini, Heath & Missiuna, 1999; Clarkin & Kendall, 1992; Goff, 1992). It is particularly difficult to determine whether one condition is in fact a symptom of the other – causality versus correlation. These important debates aside, research provides support for a number of conditions co-occurring with learning disabilities more often than expected “just by chance”.
The largest body of studies supports a comorbid relationship between learning disabilities and attention deficit disorder (with or without hyperactivity). This extensive research, featuring comorbidity estimates as high as 70%, was summarized recently by Riccio, Gonzalez & Hynd (1994) and Maynard, Tyler & Arnold (1999).
In fact, learning disabilities are sometimes confused with Attention Deficit Hyperactivity Disorder (ADHD). It is important to note that these are two distinct conditions, in spite of the significant level of co-morbidity. ADHD is not a specific learning disability. The distinguishing characteristics of students with ADHD include being more easily distracted, failing to finish assignments, weaker persistence of effort, day dreaming, looking away more often from activities they are requested to do and demonstrating less persistence of effort when completing boring activities (Barkley, Dupaul & McMurray, 1990). As well, children with ADHD have been distinguished from those with LD based on their higher levels of activity and impulsiveness. As mentioned above, a very large percentage of those who have ADHD also have accompanying learning disabilities, while approximately 30% of those who have learning disabilities also have ADHD. Nevertheless, the interventions that benefit people with ADHD and those who have learning disabilities are not the same. Therefore, it is important to diagnose these conditions accurately, before developing an Individual Education Plan for the student.
Confusion sometimes also arises for students who have learning problems arising from an acquired brain injury. While several symptoms of this condition also occur in children with learning disabilities, acquired brain injury is sometimes treated as distinct from learning disabilities. It is important to note that neither ADHD nor acquired brain injury are identified as specific exceptionalities within the Ontario educational system. As a result, many students with these conditions are included under the learning disability designation for the purposes of special education service delivery.
A group of disorders also found frequently to be comorbid with learning disabilities is that involving social, emotional, and/or behavioural difficulties (Kamphaus, Frick & Lahey, 1991; Glassberg, Hooper & Mattison, 1999). Studies suggest that anywhere from 24% to 52% of students with learning disabilities have some form of such a disorder (Rock, Fessler & Church, 1997). This group encompasses diagnoses such as conduct disorder and oppositional/defiant disorder (DeLong, 1995; Shaywitz & Shaywitz, 1991), as well as social adjustment disorder (Lyon, 1996).
Research also suggests that depressive or dysthymic disorders co-occur with learning disabilities (San Miguel, Forness & Kavale, 1996) although the nature of the relationship continues to be controversial (Wiener, 1998).
Research provides significant evidence supporting the co-morbidity of the following disorders with learning disabilities:
- Tourette’s Syndrome (Burd, Kauffman & Kerbeshian, 1992; Shady, Rulton & Champion, 1988; Chase, Friedhoff & Cohen, 1992; Walter & Carter, 1997)
- Schizophrenia (James, Mukherjee & Smith, 1996; Gillian, Johnstone, Sanderson, Cunningham & Muir, 1998);
- Epilepsy (Kerr & Espie, 1997; Espie, Kerr, Paul, O’Brien, Betts, Clark, Jacoby, & Baker, 1997; Laidlaw, Richens & Chadwick, 1993);
- Language/communication disorders (Riccio & Hynd, 1993; Schoenbrodt, Kumin & Sloan, 1997);
- Hearing impairment (Bunch & Melnyk, 1989);
- Visual disabilities (low vision, blindness) (Erin & Koenig, 1997); and
- Developmental co-ordination disorder (Missiuna, 1996; Fletcher-Finn, Elmes, & Strugnell, 1997; Martin, Heath & Missiuna, 1999)
The following are questions that you can use to see if someone may be at risk of learning disabilities. The questions should be used with individuals who show competencies in many areas, but demonstrate difficulties that cannot be explained by lack of education, low intelligence or mental health/addiction problems.
| I am going to read some statements and I want you to tell me whether they describe you at home, school or work.You can answer: Never, Sometimes, or Often | Please indicate the answer most appropriate | ||
| I remember faces but have trouble remembering people’s names |
Never |
Sometimes |
Often |
| I learn best when someone shows me what to do |
Never |
Sometimes |
Often |
| If a job is broken up into small chunks, I perform better.I have difficulty remembering the order that must be followed when I am given instructions |
Never |
Sometimes |
Often |
| I respond well to written instruction, but have trouble understanding what people are saying to me, especially when they speak quickly |
Never |
Sometimes |
Often |
| I have trouble thinking of the right word to say or write, even when I know the word |
Never |
Sometimes |
Often |
| I write well, but get confused when I’m trying to explain things to people. |
Never |
Sometimes |
Often |
| I have trouble pronouncing long words |
Never |
Sometimes |
Often |
| I am a good speaker, but when I read, the words and letters seem to jump around on the page |
Never |
Sometimes |
Often |
| I lose my place easily when I am reading |
Never |
Sometimes |
Often |
| I have trouble sounding out new words |
Never |
Sometimes |
Often |
| I can sound out words, but I don’t remember what words look like |
Never |
Sometimes |
Often |
| I remember things I hear, but misspell small words as often as big words |
Never |
Sometimes |
Often |
| I can spell the same word several ways in the same story |
Never |
Sometimes |
Often |
| I understand a story better if someone reads it to me |
Never |
Sometimes |
Often |
| I usually remember verbal instructions, but have to read things several times before I understand them |
Never |
Sometimes |
Often |
| I lose my place when copying from the blackboard or an overhead |
Never |
Sometimes |
Often |
| I organize my spoken conversation well, but my handwriting is hard for other people to read |
Never |
Sometimes |
Often |
| I express myself better when speaking than when writing |
Never |
Sometimes |
Often |
| I have trouble getting my ideas down on paper |
Never |
Sometimes |
Often |
| I have lots of good ideas in meetings, but other people don’t understand what I am trying to say in my writing |
Never |
Sometimes |
Often |
| I sometimes reverse letters or numbers, or get them in the wrong order |
Never |
Sometimes |
Often |
| I have excellent reading abilities, but trouble remembering multiplication tables |
Never |
Sometimes |
Often |
| I write well, but have trouble figuring out what they’re asking in math word problems |
Never |
Sometimes |
Often |
| I make mistakes when working through math problems that have several steps |
Never |
Sometimes |
Often |
| I can’t figure out what formulas to use in math questions |
Never |
Sometimes |
Often |
| I know what to do in math questions, but I get the calculations wrong if I don’t use a calculator |
Never |
Sometimes |
Often |
| It takes me a while to find my way around a new place |
Never |
Sometimes |
Often |
| I have trouble judging distances |
Never |
Sometimes |
Often |
| I confuse left and right |
Never |
Sometimes |
Often |
| I have trouble judging how much time tasks are going to take to complete |
Never |
Sometimes |
Often |
| I am often late getting places |
Never |
Sometimes |
Often |
| I have trouble finding things on a cluttered desk |
Never |
Sometimes |
Often |
| Jigsaw puzzles are something I’ve always avoided |
Never |
Sometimes |
Often |
| I get confused when I’m trying to do too many things at once |
Never |
Sometimes |
Often |
| I have trouble finding the right place to fill in information on forms |
Never |
Sometimes |
Often |
| I get along with people at work, but I sit by myself at lunch |
Never |
Sometimes |
Often |
| I love social gatherings, but tend to interrupt discussions |
Never |
Sometimes |
Often |
| Driving is something I have always avoided |
Never |
Sometimes |
Often |
Everyone has problems with these areas some of the time, but if there are many questions answered “often”, it may be useful to look further into the possibility of learning disabilities.
Author: Dr. Norman Brodie
Source: Adapted from an article in LDA Yukon News, June 1998, reprinted with permission of the author.
Background information
A good diagnostic assessment for learning disabilities needs to address several important areas. A primary need at the onset of the diagnostic process is the taking of a good history. While the diagnostic testing can provide excellent evaluations of the current levels of functioning in the various areas assessed, it is also important to have:· a detailed history of the development of the problems (including a developmental history with attention to issues such as delayed speech and motoric milestones)
- any family history of similar conditions amongst blood relatives (many learning disabilities “run in families” and are clearly related to genetic predispositions),
- and personal history for relevant events such as head injuries or other neurological insults and emotional stressors (such as family break – ups, exposure to domestic violence or child abuse, reactions to changes tn the family structure from additions or losses to the family, etc.)
- This background information is crucial to a thorough assessment, as the professional not only has to determine if there are true educational deficits or impairments, but also to attempt to identify the cause of them in order to determine the correct line of intervention.
The next stage of the assessment process is to obtain some current information regarding the child’s functioning in the day – to – day life situations such as at school and at home. Depending upon the age and expressive verbal skills of the child, a considerable amount of information may be obtained from a direct interview and asking specific questions about their experiences and feelings in different situations. This helps to identify how the child sees him or herself, as well as providing some insight into their self-esteem and approach to challenging situations. I also interview the parents whenever possible and generally attempt to get some additional information from both parents and the teacher through behavioural rating scales that help to quantify and make more specific the descriptions of the behavioural and emotional responses in different environments. This is especially critical when assessing for the possible presence of an Attention Deficit Hyperactivity Disorder (ADHD) and/or a Conduct Disorder, as many of the defining symptoms or problems associated with these conditions are not likely to be displayed or observed in the one – on – one testing session in the office setting.
INTELLECTUAL FUNCTIONING
In the formal testing session, it is vital to obtain reliable measures of the child’s current intellectual functioning and academic achievement as a basic prerequisite for making a diagnosis of learning disability. Intellectual testing is most commonly done using the Wechsler Intelligence Scale for Children – 3rd Edition (WlSC – Ill). This is the most widely used intellectual battery for children in North America, and it also now provides (since 1996) Canadian norms based on a very large sample of children from across Canada. The Canadian norms should generally be used as there are significant differences in performance level seen between the norms for the USA and Canada, largely indicating that the American norms tend to over – estimate the child’s performance by a slight extent compared to standards in Canada.
The WISC – III is also a very useful test because it not only provides a general estimate of learning aptitude, it also provides a breakdown into the areas of Verbal, Performance (nonverbal) and Full Scale I.Q. It is also possible to identify patterns of strength and weakness across the profile that can help with determining more specific diagnoses of subtypes of learning disability (such as the identification of global language disorders or nonverbal learning disability subtypes) by consideration of discrepancies between the Verbal and Performance I.Q. scores and patterns of strength and weakness on the subtests.
ACADEMIC ACHIEVEMENT
In combination with the intellectual test results, it is also important to obtain concurrent measures of academic achievement using standardized tests that provide reliable estimates of performance relative to age or grade population norms. This allows for a comparison of performance using national standards rather than subjective ratings based on a comparison to the rest of the child’s class (with uncertainty as to how he/she would compare to a different class of students). It also provides an objective basis for comparing performance to potential by contrasting standard scores from the achievement test (which are generally expressed in I.Q. like units) with the I.Q. scores to determine if the achievement level is significantly below the intellectual expectancy range. This is important in that all standard definitions of learning disability emphasize that the individual has a deficit in learning that is not attributable to general intellectual handicap or deficiency.
It is also important to consider the possibility that a very bright child who functions in the well above average range on the intellectual battery may still have a significant learning disability condition that results in a relative deficit on academic achievement as reflected by low to even mid – average performances on the achievement tests. Formal assessment of academic achievement levels with standardized tests is also important with respect to qualifying for special education assistance in most jurisdictions in Canada. Most education departments have set quantified criteria for identification of learning disability based on performing below specific levels (often at below the 10th percentile) on one or more academic test areas, using a recognized educational achievement test.
Some of the most commonly used educational batteries include:
- the Woodcock – Johnson Psycho – Educational Battery – Revised (WJ – R)
- the related Woodcock Reading Mastery Test – Revised (WRMT – R)
- the Kaufman Test of Educational Achievement (K – TEA)
- the Wechsler Individual Achievement Test (WIAT)
- the Wide Range Achievement Test – 3rd Edition (WRAT – 3)
- and the Canada Quick Individual Achievement Test (C – QUIET)
Each of these tests employs a battery approach to educational testing, employing a number of individual subtests that assess specific skill areas, allowing for the performance to be compared across subject or skill areas, and providing normative data that allows the individual’s scores to be compared to standards established at a national level. All of these tests also correlate quite highly with one another, and the results obtained on one tend to be similar to the results obtained on another, such that selection of the specific test is often a matter of personal preference by the specific consultant.
In my own practice, I most often employ a combination of the WRAT – 3 and C – QUIET tests in combination with other measures as needed, such as the use of the Canada French Immersion Achievement Test (C – FIAT) that is produced by the authors of the C – QUIET to allow for a direct comparison of the student’s performance levels in English and French when the child has been enrolled in a French Immersion school programme. I also employ a variety of more selective tests such as specific tests of reading vocabulary and reading comprehension from the Gates – MacGinitie Reading Tests or measures of visual spelling recognition and resistance to various forms of reading errors with the Diagnostic Analysis of Reading Errors test or measures of writing skills using the Test of Written Language – 3rd Edition. The specific test battery selected is, however, of less importance than ensuring that the areas of identified academic weakness are systematically assessed with a reliable and valid achievement test. The test should provide standard scores and percentile rankings that can be contrasted to the intellectual estimates in order to identify discrepancies indicative of learning disability, and provide a breakdown of scores into functional areas for remedial planning purposes.
SELF-ESTEEM & EMOTIONAL STATUS
Another area that should be included in almost all psycho – educational assessments is a systematic evaluation of self – esteem and emotional status. Many students with learning disabilities have developed significant problems with self – esteem and emotional reactions to prolonged frustration. Negative self – esteem and childhood depressive reactions also seriously compromise the individual’s ability to apply themselves to programming in an effective fashion. Therefore, when such emotional interferences are present (whether as a primary problem or as a secondary reaction to the learning disability), it is imperative that we recognize these as problems in their own right and initiate some intervention or provide assistance to help them begin the process of developing improved self – confidence (e.g. encouraging the child to participate in some extracurricular activities for self – esteem boosting success and “setting them up for success” in some areas). In some cases, the emotional distress and disturbance may be of sufficient severity that formal professional counselling and/or medical treatment of depression may be necessary. A combination approach of rebuilding self – esteem as well as improving the educational programming at the same time is most often necessary and critical for either aspect of the overall plan to succeed.
Summary
What is most important is for the psychologist to be able to use the available information arising from the history, clinical interviews, test behavioural observations and objective test data to achieve an integrated or holistic picture of the individual and the specific needs for each case. Only with such a well detailed picture of the person as an individual can we begin to identify specifically what type of educational programme, supplementary assistance and educational modifications are appropriate for the specific situation. This places the psychological assessment findings well above the assignment of a simple label or diagnostic term. Through such a comprehensive evaluation process, the individual’s strengths and talents are also highlighted and brought into focus as a basis for preserving and enhancing self – esteem and personal development.
Author: Yona Reznick, Art Therapist DTATI, Hons. BA
Source: reprinted with permission from the author
For individuals with learning disabilities, life can present many challenges. Looking beyond the academic, physical, and social difficulties, individuals with learning disabilities frequently experience emotional struggles. Studies have shown that lowered self-esteem, depression, and increased feelings of loneliness, stress, and anxiety are common experiences for individuals with learning disabilities. Art therapy can help reduce these negative feelings, while increasing an individuals’ self-awareness, and improving their overall emotional wellbeing.
Art therapy is a mental health service that combines the use of art and discussion in order to provide its participant with a non-verbal form of expression. Art therapy combines the tried-and-true methods of psychology with the creativity and exploration of art making, and can take place in both a group and individual therapy setting. Through the use of art in a therapeutic environment, the individual is given an opportunity to explore his or her feelings openly and creatively with the support of a professionally trained art therapist.
As an art therapist, I have dedicated myself to helping children and adolescents with learning disabilities. I have seen first-hand the power that art therapy has to increase an individuals self-esteem, to reduce their anxiety and frustration, and to improve their relationships. If you are interested in further information about art therapy, and how it can help yourself, or someone you know, please contact me at yonareznick@rogers.com.
Having a specific learning disability is an inherent, life long condition that can affect friendships, school, work, self-esteem or daily life. Many adults with learning disabilities have graduated from high school, college, trade schools or university, becoming successful in business, the arts or in their chosen profession. But for many, success has not been easy. Even though they are intelligent, some adults are conditioned to believe that they are stupid, lazy and defeated, resulting in frustration, disappointment, low self-confidence and failure.WHAT IS A LEARNING DISABILITY?It is a disorder that affects individuals of potentially average to above average intelligence by interfering with the central nervous system and its ability to process information. Learning disabilities affect the way in which an individual takes in, remembers and understands information, as well as how an individual expresses that knowledge.Some adults may experience problems in one or more of these general areas:
Memory Reasoning Coordination Communication Social Competence
COMMON SIGNS AND CHARACTERISTICS
Adults with learning disabilities may excel in the following areas:
Imagination
Creativity
Motivation
Perseverance
Spoken language
Verbal information
Visual information
Mathematics
Or they may have difficulty in the following areas:
Reading, writing, spelling, communicating and calculating
Following written instructions
Expressing ideas in writing
Completing job application forms
Finding or keeping a job
Budgeting and managing money
Managing time and activities
A short attention span, restlessness or hyperactivity
Carrying out simultaneous tasks
Remembering and following the sequence of instructions
Breaking tasks down into segments
Following verbal instructions
Understanding appropriate social behaviour
Poor coordination and spatial disorientation
Classification and organization of information
Problem solving strategies
HOW MANY PEOPLE HAVE LEARNING DISABILITIES?
You are not alone! Learning disabilities affect approximately 1 out of every 5 to 10 people. This is more than 2 million Canadians.
IS IT TOO LATE?
Before 1980, very little was done to help adults with learning disabilities. What can you do? If solid coping skills and compensatory strategies are not developed, the learning disability may continue to interfere with work, education and social relations. By developing skills and taking advantage of new technologies adults with learning disabilities will be able to succeed. Remember, it is never too late to ask for help.
USING SUCCESSFUL STRATEGIES
You can make a difference by taking control of your life and achieving your potential.
Develop coping strategies
Know and manage your specific learning disability
Find other adults with learning disabilities for sharing strategies and information
Be assessed by a professional trained in learning disabilities (neuro-psychologist, educational psychologist, etc.)
Get counselling
Develop your self-esteem through your strengths
Set goals based on your abilities
Know and use technology to compensate for weaknesses
Know your legal rights
THINGS TO REMEMBER
Having a learning disability is a condition for life
You are not alone
Support and information is available
Celebrate your uniqueness
Never give up
Reprinted with permission from Learning Disabilities Association of Quebec
(Written in collaboration with adults having learning disabilities)
Learning Disabilities (LDs) are very common and affect 5 to 10 percent of Canadians.
LDs are brain-based problems that affect one or more ways that a person takes in, stores or uses information. LDs can interfere with learning basic skills such as reading, writing, and math. They can also interfere with higher level skills such as organization, time management and social skills.
People with LDs are intelligent and can learn. The difficulties they experience are due to impairments in one or more of the psychological processes related to learning:
- Phonological processing (identifying and manipulating speech sounds)
- Working memory (holding information in mind while also using the information)
- Processing speed (speed of taking in, using or pulling out information)
- Language processing (understanding and express information using words)
- Visual-spatial processing (perceiving or organizing visual information)
- Executive functions (planning and organizing)
- Visual-motor processing (carrying out hand-eye activities)
LDs come in many forms and their effects are different from person to person. They relate to:
- Getting information into the brain (Input)
- Making sense of this information (Organization)
- Storing and retrieving information (Memory)
- Getting information back out (Output)
LDs are a life-long condition that affects people differently depending on the situation. In order to find good, effective strategies for compensating and success we need to understand how a person’s learning profile interacts with their environment.
What do LDs affect?
No two LDs are the same. LDs vary greatly in form and intensity, and can affect one or more of the following areas.
Daily life:
People with LDs may experience problems in any of the following areas:
- Organizing
- Managing time
- Planning & decision making
- Problem solving
- Learning to drive
- Seeing the “whole picture” or knowing what details are important
- Finding their way in an unfamiliar environment
- Interpreting graphs, charts and maps
- Following multi-step instructions
- Finding things on a cluttered desk
Social Life:
People with LDs may experience problems with social situations in any of the following areas:
- Interpreting facial expressions
- Understanding body language
- Understanding tones of voice
- Taking turns in conversations
Academics:
People with LDs may experience problems with reading (sometimes called dyslexia) in any of the following areas:
- Breaking words down into their individual sounds
- Recognizing words
- Reading fluently
- Understanding what is read
People with LDs may experience problems with writing (sometimes called dysgraphia) in any of the following areas:
- Handwriting
- Putting thoughts on paper
- Organizing written work
- Spelling and grammar
People with LDs may experience problems in math (sometimes called dyscalculia) in any of the following areas:
- Learning number facts
- Doing arithmetic and calculation
- Using symbols in math
- Understanding visual–spatial relationships
What does the term Nonverbal Learning Disabilities Mean?
Some people use the term Nonverbal LDs (NLD or NVLD) to describe a group of people who learn best by using words, but may experience problems in any of the following areas:
- Understanding visual spatial relationships
- Solving problems
- Understanding time
- Understanding social cues
- Math, science and writing
- Motor skills (related to printing and writing
What can it feel like to have LDs?
LDs can affect people differently depending on what they understand about their LDs, and what supports they have in their environment. People may struggle with:
- Feeling frustrated with not being able to do what people expect of them
- Having difficulty keeping up with their class mates, co-workers or friends
- Feeling shame about having a disability
- Experiencing a lack of understanding from the people in their lives
- Being the target of bullies
These situations may lead to:
- Low self-esteem
- Lack of confidence
- Feeling dumb
- A sense of failure
- Appearing less motivated
- Loneliness
- Social withdrawal
Not all individuals with LDs have social, emotional or behavioural problems. About 40% of people with LDs experience mental health difficulties such as anxiety and depression.
What Helps?
Most people with LDs are resilient, and learn to manage challenges and achieve success. There are a number of factors that help. These include:
- Understanding their LDs and what helps them learn
- Learning how to set realistic goals, to solve problems and to make good choices
- Being open to asking for and getting help
- Not giving up when things get hard
- Believing successes are due to their own efforts
- Believing they can learn from their mistakes
- Feeling respected and connected to others
- Having someone who will listen to them and understand their feelings
- Being an active member of a community or group
LDs are complicated, helping isn’t. We all can help by:
- Showing understanding and encouragement
- Recognizing small successes
- Learning more about LDs
From a brochure, What are Learning Disabilities?, developed by the Learning Disabilities Association of Ontario, www.LDAO.ca, and the Integra Program (now of the Child Development Institute), www.childdevelop.ca/programs/integra-program.
Author: Catherine M. Smith
Source: Reprinted with permission from LDAC’s newsletter National.
First, the good news. Most people who have learning disabilities heave a sigh of relief when school days are finally behind them and get on with satisfying, successful lives. They find a niche where they can fit into the workforce, matching their skills and abilities to the right job. Many are college and university graduates, and take their places confidently and comfortably in their chosen fields.
Now, the less good news. Many people who have learning disabilities struggle to get appropriate training or education, struggle to find jobs, struggle to get accommodations in the workplace, or get jobs only to lose them within a short time. There are several possible reasons for this: lack of fit between skills and job requirements; social skills difficulties; systemic barriers resulting in lack of appropriate accommodations; and difficulty handling the learning experiences inherent in any job in today’s world.
Fit, between skills and jobs is a primary ingredient for success. This is true for everyone. For individuals who have learning disabilities it means that they must have a clear understanding of their specific learning disabilities and understand when and how they are likely to manifest. Many individuals leave high school with only the vaguest general idea of what their deficit areas are, and little idea of how those will impact on various career possibilities. For example, I have worked with an individual who struggled mightily to get through law school. She finally succeeded. However, her main area of difficulty was auditory processing deficits. Her score on a standardized test placed her well below the 16 th percentile. This is a major handicap for a lawyer whose job is to process accurately and remember large amounts of information. When I tried to reach her at her business number a year or so after her graduation, it was out of service. I do not know that she was not able to make it as a lawyer, but it would surprise me greatly if she did. On the other hand, I worked with a young man at university who had great difficulties with writing. He was in an applied program of video production in which his strengths were utilized and the need for writing was minimal. This represents a good “fit” between strengths and job requirements. He had all the part-time work he could handle in his field and would likely have no difficulty achieving success as a full-time worker.
Some individuals with learning disabilities have social skills deficits. They have difficulty reading social situations, understanding the non-verbal aspects of communication (tone of voice; pace of delivery; non-word vocalic such as “um, ah, oh”; body position and gestures; facial expressions), using eye contact appropriately, listening, asking for help, explaining a problem, accepting ‘no’ for an answer, and turn-taking in conversations. The Conference Board of Canada has published a leaflet called Employability Skills Profile . It lists the general skills that all employers look for and value in all employees. A look at this list of Critical Skills Required for the Workforce makes it clear why individuals with social skills deficits have difficulty succeeding in the workplace even if they have the requisite hard job skills. The list of ‘critical skills’ includes the abilities to: listen to understand and learn; understand and contribute to the organization’s goals; understand and work with the culture of the group; plan and make decisions with others and support the outcome; respect the thoughts and opinions of others in the group; exercise “give and take” to achieve group results; seek a team approach as appropriate; and lead when appropriate, mobilizing the group for high performance. A survey of employers conducted by the Ontario Ministry of Labour revealed that they cite ‘lack of social skills’ as the main reason for termination of employment. This makes social skills deficits a serious issue for people with learning disabilities who have this particular deficit.
Individuals who have social skills deficits can learn to perform many of the skills mentioned as essential. They do not learn automatically, but they need to have each skill made explicit, have the skill demonstrated, and practice the skill in a supportive environment receiving corrective feedback. They often need ongoing ‘remediation’ to help them apply the skills they have learned when they are actually in the workplace. Social skills training is best done in small groups where students can help each other as they are learning under the guidance of a trained facilitator.
Even those who have good job skills and good social skills may run into systemic barriers. This refers to practices or attitudes within the workplace that work to prevent individuals from achieving success. Such practices or attitudes preclude implementation of accommodations that would enable people to do their work effectively. Our Charter of Human Rights and Freedoms, and associated Human Rights Acts dictate that accommodations must be provided to individuals with disabilities. In order to refuse a job to, or let go, a person for lack of ability to do the job, the employer first must make sure the individual cannot do the job even with appropriate accommodations . Accommodations include such things as assistive technology (voice interactive software), job restructuring (if there is one minor aspect of the job that cannot be performed even with accommodations, giving that part of the job to another individual in exchange for something the person can do), providing written instructions for workers with memory problems; and allowing extra time for new skills required for the job to be learned. A recent case that went to trial involved an individual who was denied a promotion because it took her longer to achieve a second-language proficiency requirement. After many years, the individual won her case. But how many people are there who do not have the time, motivation, or resources to fight such a battle, and therefore simply accept the discrimination?
Paul Gerber and his colleagues who have spent years researching adults with learning disabilities, have looked at the positive side of employment by interviewing many highly and moderately successful adults with learning disabilities. They concluded that the overriding issue mitigating for success was the quest by individuals to gain control over their lives. Control was pursued through two sets of themes: internal decisions and external manifestations.
The internal decisions included having the desire to succeed, being goal-driven, and having reframed how learning disabilities was thought about. Having the desire to succeed is quite straight forward. Everyone I have ever met has that desire. It becomes trickier when self-efficacy enters the picture. Self-efficacy refers to one’s belief that one’s own efforts have a direct impact on outcomes. Many people with learning disabilities do not believe that what they do makes any difference…they will either succeed or not, depending on luck, their teacher, their boss, or other factors apart from their own effort. Those who succeed want to succeed and believe that what they do makes the difference. Therefore they are more motivated to take action and persevere. At some point, adults with learning disabilities who achieve success decide to take control over their own lives and make things happen by taking direct action.
All of the successful adults interviewed by Gerber and his colleagues routinely set goals, both long-term and short-term. It is important that the goals be realistic, that is, achievable. Goals that are too easy are not meaningful as motivators. Goals that are unrealistic in light of the individual’s strengths and weaknesses are not likely reachable and so serve to de-motivate rather than motivate. But clear, achievable goals, accompanied by a plan of action, serve to propel individuals toward success. Strategic thinking becomes important if goal-setting is to work. Success or failure to reach goals needs to be accompanied by reflection about why the individual succeeded or not, and if not, what other strategy could be tried. This type of strategic thinking does not come naturally to many individuals with learning disabilities. Deborah Butler has developed a method to help college students learn to think strategically by repeatedly leading them through the cycle of goal-setting, plan development, plan implementation, and reflection.
The third internal decision identified by Gerber was reframing . That is the process of recognizing and accepting the impact of the learning disabilities and accepting and valuing oneself, including the learning disabilities. It means making friends with one’s learning disabilities, and approaching life with a positive attitude. Such acceptance brings with it the ability and willingness to discuss one’s learning disabilities with others when and as appropriate, without shame or guilt. In order to be able to do so, individuals need to truly understand their own strengths and weaknesses so they can be dealt with realistically when making career decisions or discussing the need for accommodations. The final stage in the reframing process is action : taking direct action toward goal achievement.
Having made these internal decisions, successful individuals then exhibit behaviours that are consistent with those decisions. They select jobs or careers which fit well with their abilities and disabilities, persist in their efforts to achieve success, and become creative in developing or learning new strategies to help them get around their areas of difficulty. To do this, many develop a solid network of friends, supporters, mentors, and learning experiences/resources that may be called upon when required. Learning how to make effective use of technology would fall into this category. Developing the ability and willingness to seek out and accept support is key.
A very pragmatic question often arises for individuals with learning disabilities. “When should I disclose to an employer that I have learning disabilities?” There is no stock answer to this question. If the individual’s learning disabilities are not expected to be an issue in the particular job, there is no need to disclose. For example, a person may have arthritis, diabetes, or depression. If the condition is under control and not likely to surface as a barrier to that individual’s effective job performance, then it is a non-issue and does not need to be disclosed. If, however, the condition is not well controlled and is likely to interfere with the individual’s ability to carry out all aspects of the job effectively, then the condition needs to be disclosed and adaptations identified to deal with the issues. The same is true for learning disabilities. The more one has chosen work that provides a good fit with individual strengths and weaknesses, the less likely it is to be an issue. If it is an issue, it needs to be disclosed before work commences, but after the job offer has been made. This allows the individual to identify strategies and adaptations which will permit effective job completion, or allows the employee and employer to work together to find workable solutions. The bottom line always must be that the employee can perform the essential elements of the job with adaptations. If the essential elements of the job cannot be performed, even with adaptations, there is no ‘fit’, and the employer needs to find another person who can do the job. The potential employee needs to find work or a job where there is a fit. Happily, recent court decisions have made it clear that the onus is on employers to prove that every avenue has been tried to make jobs work for individuals with learning disabilities before refusing to hire or promote, or terminating employment.
In school, students with learning disabilities vary greatly in their need for support. Some need a special school, some a special class, some resource support, and some cope nicely without any special supports. In the workplace, the same is true for adults. Some require significant rehabilitation programs to prepare them for success in the workplace. Such a program could include assessment, remediation, career assessment and counselling, skills training with proper adaptations, on-the-job training, unpaid work placement with monitoring, coaching, or counselling, and social skills training. Some require access to education and training with adaptations provided. Some only need employers willing to provide adaptations in the workplace. And some perform with no special supports. Hopefully this article offers guidance to help you, or your loved one, make decisions about what, if anything, is needed.
In this article, the term learning disabilities includes attention deficit/hyperactivity disorder.
Source: Adapted with permission from an article by Patti Brace in LDA of Kingston Newsletter
Nonverbal learning disabilities (NLD) are less well known than language-based learning disabilites such as dyslexia.
Typically, people with nonverbal learning disabilities show:
- excellent memory for things they hear
- poor memory for things they see
- good reading ability
- very poor arithmetic ability
- excellent verbal expression and verbal reasoning
- problems with written expression (often because of poor handwriting)
- problems with sense of direction, estimation of size, shape, distance
- problems reading facial expressions, gestures, social cues, tones of voice
Nonverbal learning disabilities often go undiagnosed because reading ability tends to be regarded as the chief indicator of academic well-being by most public school systems. Because it has a pronounced effect on social interaction, as well as academic performance, nonverbal learning disabilities present a unique challenge to parents, teachers and adult consumers.
The chief characteristics of nonverbal learning disabilities include:
- tactile-perceptual deficits, usually on the left side of the body
- coordination difficulties, again often more marked on the left side of the body
- problems with visual-spatial organization
- extreme difficulty adapting to new and complex situations
- reliance on rote behaviours (which may or may not be appropriate) in new situations
- trouble understanding nonverbal feedback in social situations
- problems with social perception, social judgement and social interaction
- distorted sense of time
- very strong rote verbal abilities (e.g. large vocabulary)
- reliance on language as the primary means for social relating, information-gathering and relief from anxiety
- difficulties with arithmetic and, later, with scientific concepts and theories
- inattention and hyperactivity earlier in childhood; and social withdrawal and isolation later
When people with nonverbal learning disabilities are assessed, typically, their performance IQ is significantly lower than their verbal IQ, because of visual-spatial weaknesses.
Young Children
Young NLD children tend to stray from home or groups and get lost easily. They often spill things at mealtime because of problems with motor coordination and have trouble dressing themselves for the same reason. Problems with spatial skills appear in a weak understanding of nonverbal information (e.g. pictures, cartoons, passage of time) and nonverbal tasks like puzzles.
Many children with NLD use words in an adult fashion and learn to read before school age because of their auditory strengths. Thus, they often try to gain information about the world around them by asking endless questions of adults rather than by exploring on their own. The inaccuracy of their visual perception, physical awkwardness and difficulty integrating information in space and time make it harder for them to make sense of the physical world. This compensation can compound the problem, however, for the less the child engages in physical exploration, the less she/he learns about relationships between objects in space.
Academic Issues
Students with NLD generally appear to possess above-average cognitive skills because of their verbal strengths, but often show academic difficulties as they reach secondary levels.
Spatial and coordination problems make printing and writing, learning math, telling time, reading and colouring maps and keeping one’s place on the page difficult from early grades. By secondary school more complex verbal language is based on nonverbal processes like spatial relationships (in science, for example), logical ordering, and sequencing (both skills necessary for writing essays.) This can cause problems in subject areas other than math. For example, students often experience difficulties with sense of time, arranging written material on a page, making change, and sewing and typing, all of which demand good spatial awareness.
Throughout the school years, children with NLD are often inattentive and poorly organized because they have trouble integrating and interpreting incoming information. They tend to pay attention to each detail as it comes in, rather than combining them into more meaningful wholes. The effort quickly leads to information overload, with which these students will often cope by clinging to familiar habits and routines that help them to structure their world. Sometimes this means of coping appears as misbehaviour.
In later secondary and post-secondary education, information is frequently presented in lecture form. For students with NLD, problems arise because they have to integrate information they hear with the act of writing, already difficult because writing is often awkward and slow. In addition, students who attend equally to individual details as they appear have enormous difficulty separating important from unimportant information.
Teachers can support students with NLD by outlining material to be covered, using overheads containing central points while lecturing, providing clear schedules of the day’s events, breaking down complex tasks into smaller, sequenced pieces, using discussion rather than lectures to develop and integrate ideas, and using students’ strengths in rote learning to help them develop habits and routines to organize themselves and their work.
Social and Emotional Issues
Possibly the biggest area of concern for children and adults with NLD is social skills. One result of having trouble processing nonverbal and spatial information is missing or misinterpreting subtle social cues like facial expressions, gestures and tones of voice. For example, a phrase like “nice going” means something different when you’ve just dropped a ball or tripped over a skipping rope (again) than when you’ve gotten a perfect score on a spelling test. Confusing the two can spell “disaster” on the playground.
Unlike a student who has difficulty reading but does well with social and sports activities, students with NLD are affected in all areas. This can lead to social isolation which children will sometimes try to alleviate by interacting only with adults, who are more appreciative of their verbal strengths and less concerned about physical awkwardness or violations of social conventions. However, because children with NLD are highly verbal, parents and teachers tend to attribute their academic and social failure to laziness or poor character. This can lead to emotional problems like depression and anxiety that may be expressed in physical ways (e.g. nail and cuticle biting, headaches, stomach problems, phobias).
Parents and teachers can help children with NLD learn more effective social skills by talking about social rules and playing games in which children guess the feelings that go with facial expressions and tones of voice, and figure out appropriate responses. Friends and spouses of adults with NLD can help by pointing out social rules and articulating the information often carried by a look or a gesture.
References
- Gross-Tsur, Varda et al. “Developmental Right-Hemisphere Syndrome: Clinical Spectrum of the Nonverbal Learning Disability”. Journal of Learning Disabilities, February 1995.
- Harnadek, Michael and Byron P. Rourke. “Principal Identifying Features of the Syndrome of Nonverbal Learning Disabilities in Children”. Journal of Learning Disabilities, March 1994.
- Humphries, Tom. Nonverbal Learning Disabilities: A Distinct Group Within Our Population. Communique (LDA Ontario), Autumn 1993.
- Moss-Thompson, Owinda. “The Nonverbal Dilemma”. Journal of Learning Disabilities 1985.
- Rourke, Byron. “Nonverbal Learning Disabilities: Development of the Syndrome and the Model”. News & Events (LDA Nova Scotia), February 1997.
Author: G. Reid Lyon, Ph.D
Source: reprinted with permission from The International Dyslexia Association’s Quarterly Periodical, Perspectives, Spring 2003
The National Institute of Child Health & Human Development (NICHD) considers that teaching and learning in today’s schools reflect not only significant educational concerns, but public health concerns as well. Our research has consistently shown that if children do not learn to understand and use language, to read and write, to calculate and reason mathematically, to solve problems, and to communicate their ideas and perspectives, their opportunities for a fulfilling and rewarding life are seriously compromised. Specifically, in our NICHD-supported longitudinal studies, we have learned that school failure has devastating consequences with respect to self-esteem, social development, and opportunities for advanced education and meaningful employment. Nowhere are these consequences more apparent than when children fail to learn to read. Why? Simply stated, the development of reading skills serves as THE major foundational academic ability for all school-based learning. Without the ability to read, the opportunities for academic and occupational success are limited. Moreover, because of its importance, difficulty in learning to read crushes the excitement and love for learning, which most children have when they enter school.
As we follow thousands of children with reading difficulties throughout school and into adulthood, these young people tell us how embarrassing and devastating it was to read with difficulty in front of peers and teachers, and to demonstrate this weakness on a daily basis. It is clear from our NICHD research that this type of failure affects children negatively earlier than we thought. By the end of first grade, children having difficulty learning to read begin to feel less positive about their abilities than when they started school. As we follow children through elementary and middle school, self-esteem and the motivation to learn to read decline even further. In the majority of cases, the students are deprived of the ability to learn about literature, science, mathematics, history, and social studies because they cannot read grade-level textbooks. Consider that by middle school, children who read well read at least 10,000,000 words during the school year. Children with reading difficulties read less than 100,000 words during the same period. Poor readers lag far behind in vocabulary development and in the acquisition of strategies for understanding what they read, and they frequently avoid reading and other assignments that require reading. By high school, the potential of these students to enter college has decreased substantially. Students who have stayed in school long enough to reach high school tell us they hate to read because it is so difficult and it makes them feel “dumb.” As a high school junior in one of our studies remarked, “I would rather have a root canal than read.”
It is important to note that this state of educational affairs describes an extraordinary and unacceptable number of children. According to the National Center for Educational Statistics (1998), 38% of fourth graders nationally cannot read at a basic level – that is, they cannot read and understand a short paragraph similar to that in a children’s book. Unfortunately, reading failure is disproportionately prevalent among children living in poverty. In many low-income urban school districts the percentage of students in the fourth grade who cannot read at basic level approaches 70%.
The educational and public health consequences of this level of reading failure are dire. Of the 10 to 15% of children who will eventually drop out of school, more than 75% will report difficulties learning to read. Likewise, only two percent of students receiving special or compensatory education for difficulties learning to read will complete a four-year college program. Approximately half of children and adolescents with a history of substance abuse have reading problems. Failure to learn to read places children’s futures and lives at risk for highly deleterious outcomes. For this reason the NICHD considers reading failure to reflect a national public health problem.
How Reading Develops, and Why So Many of Our Children Have Difficulty Learning to Read
Converging scientific evidence from studies supported by NICHD indicates that learning to read is a relatively lengthy process that begins before children enter formal schooling. Children who receive stimulating oral language and literacy experiences from birth onward appear to have an edge when it comes to vocabulary development, developing a general aware-ness of print and literacy concepts, understanding and the goals of reading. If young children are read to, they become exposed, in interesting and entertaining ways, to the sounds of our language. Oral language and literacy interactions open the doors to the concepts of rhyming and alliteration, and to word and language play that builds the foundation for phonemic awareness – the critical under-standing that the syllables and words that are spoken are made up of small segments of sound (phonemes). Vocabulary and oral comprehension abilities are facilitated substantially by rich oral language inter-actions with adults that might occur spontaneously in conversations and in shared picture book reading.
However, the experiences that help develop vocabulary and general language and conceptual skills in preschoolers are different from the experiences that develop specific types of knowledge necessary to read, including knowledge about print, phonemic awareness, and spelling. These skills need to be systematically and, depending upon the level of the child’s background knowledge, explicitly taught. Preschool children who can recognize and discriminate letters of the alphabet are typically from homes in which materials such as magnetized letters and alphabet name books are present and are the source of teaching interactions with parents. Clearly, these children will have less to learn when they enter kindergarten. The learning of letter names is also important because the names of many letters contain the sounds they most often represent. With this knowledge, the child is oriented to what is termed “the alphabetic principle” – a principle that explains how sounds of speech (phonemes) become associated with letters of the alphabet (phonics). This principle stands at the core of learning and applying phonics skills to print.
Ultimately, children’s ability to comprehend what they listen to and what they read is inextricably linked to the depth of their background knowledge. Very young children who are provided opportunities to learn, think, and talk about new areas of knowledge will gain much more from the reading process. With understanding comes the desire to read more. Thus, ensuring that reading practice and the development of new vocabulary takes place. Through these early interactions and the systematic exposure to language and literacy concepts provided by parents, caregivers, and teachers, skilled readers learn to apply phonemic and phonics skills rapidly and accurately. Children that practice reading develop fluency, automaticity, and the ability to read with expression, and to apply comprehension strategies to what they are reading to facilitate understanding. It all starts very early, with those initial language and literacy interactions that expose the child to the structure of our language and how print works.
Unfortunately, few children who later have difficulties learning to read, and particularly children from poverty, come to kindergarten and the first grade with these advantages. We know that the average middle class child is exposed to approximately 500,000 words by kinder-garten; an economically disadvantaged child is exposed to half as many, at best.
In essence, children who are likely to have difficulties learning to read can be readily observed in the initial stages of their literacy development. They approach the reading of words and text in a laborious manner, demonstrating difficulties linking sounds (phonemes) to letters and letter patterns. Their reading is hesitant and characterized by frequent starts, stops, and mispronunciations. Comprehension of the material being read is usually extremely poor. However, it is often not because he or she is not smart enough. In fact, many children who have difficulty learning to read are bright and motivated to learn to read – at least initially. Their difficulties understanding what they have read occur because it takes far too long to read words, leaving little energy for remembering and comprehending what was read. Unfortunately, the slow and inaccurate reading of words cannot be improved in any appreciable way by using the context of what is read to help pronounce the words correctly. Consequently, while the fundamental purpose of reading is to derive meaning from print, the key to comprehension starts with the rapid and accurate reading of words. In fact, difficulties in decoding unfamiliar words and learning to recognize words rapidly are at the core of most reading difficulties. These difficulties can be traced systematically to initial difficulties in understanding that the language that is heard by the ear is actually composed of smaller segments of sound (e.g., phonemic awareness). And here we come full circle – many of these early difficulties in developing phonemic awareness are due to a lack of literacy and oral language interactions with adults during infancy and early childhood. Thus, because the environments most bereft of these interactions are those characterized by poverty, the cycle continues.
Can Children with Reading Problems Overcome Their Difficulties?
Yes, the majority of children who enter kindergarten and elementary school at-risk for reading failure can learn to read at average or above levels, but only if they are identified early and provided with systematic, explicit, and intensive instruction in phonemic awareness, phonics, reading fluency, vocabulary, and reading comprehension strategies. Substantial research supported by NICHD shows clearly that without systematic, focused, and intensive interventions, the majority of children rarely “catch up.” Failure to develop basic reading skills by age nine predicts a lifetime of illiteracy. Unless these children receive the appropriate instruction, more than 74% of the children entering first grade who are at-risk for reading failure will continue to have reading problems into adulthood. On the other hand, the early identification of children at-risk for reading failure coupled with the provision of comprehensive early reading interventions can reduce the percentage of children reading below the basic level in the fourth grade (i.e., 38%) to six percent or less.
Are Certain Reading Instructional Approaches More Effective Than Others?
Yes. On the basis of a thorough evidence-based review of the reading research that met rigorous scientific standards, the National Reading Panel (NRP), convened by the NICHD and the Department of Education, found that instructional programs that provided systematic instruction in phonemic aware-ness, phonics, guided repeated reading to improve reading fluency, and direct instruction in vocabulary and reading comprehension strategies were significantly more effective than approaches that were less explicit and less focused on the reading skills to be taught (e.g., approaches that emphasize incidental learning of basic reading skills). The NRP found that children as young as four years of age benefited from instruction in phonemic awareness and the alphabetic principle when the instruction was presented in an interesting and entertaining, albeit systematic manner. Likewise, the National Center for Educational Statistics recently reported data from its Early Childhood Longitudinal Study involving 22,000 children showing that, after controlling for family income, youngsters who attended more academically oriented preschool programs had significantly higher scores in reading, math, and general knowledge when tested in the fall of their kindergarten year than children attending less academically oriented preschools. Five NICHD longitudinal early intervention studies have examined the effectiveness of different early intervention approaches provided in kindergarten and first and second grades for those children most at-risk for reading difficulties. These studies strongly suggest that such programs if implemented appropriately, could reduce the number of children who fail to learn to read well below the 38 % rate currently observed nationally. It is also important to note that the majority of children composing this unacceptably large group of poor readers ARE NOT provided special education services, as is discussed next.
Will Effective Reading Instruction Reduce the Need for Special Education?
That is possible in the long run. What is now clear is that effective instruction will help differentiate between children whose reading problems are related to inadequate instruction (curriculum casualties) versus children who continue to struggle despite early and intensive instruction. The number of children with reading difficulties served in special education reflects only a fraction of the number of school-age children who fail to learn to read. Recall from the previous discussion that approximately 38 % of fourth grade students read below the basic level. Keeping in mind that the majority of these children will continue to have reading difficulties throughout their school career if they do not receive systematic and focused early intervention, we can estimate that at least 20 million school-age children suffer from reading failure. Among these 20 million children, only approximately 2.3 million school-age children are served in special education under the category of Specific Learning Disabilities (SLD). The remaining 17.7 million poor readers not meeting the eligibility requirements for the SLD category are either provided some form of compensatory education or overlooked all together.
We have taken care in our NICHD early intervention and prevention studies to identify ALL children who are at-risk for reading failure within a given sample and to identify the instructional approaches that are the most effective for the majority of these students, irrespective of whether they are eligible for special education. As noted earlier, these studies have indicated that, with the proper early instruction, the national prevalence of reading failure can be reduced significantly. Thus, by putting in place well designed evidence-based early identification, prevention, and early intervention programs in our public schools, our data strongly show that the 20 million children today suffering from reading failure could be reduced by approximately two-thirds. While still a totally unacceptable rate of reading failure, such a reduction would allow us to provide services to the children who are in genuine need of special education services with substantially greater focus and intensity.
Our challenge now is to close the gap between what we know works from research and the ineffective practices that many prospective teachers are taught during their preparation and the ineffective instruction still being provided in most of our nation’s classrooms. The question is, do we have the courage to do so?
Understanding Dyslexia
Dyslexia is a learning disability involving difficulties with different forms of language. These can include problems with reading, spelling, understanding spoken language and/or expressing oneself in speaking or writing.
Dyslexia, like other learning disabilities, is not related to intelligence. An unexpected gap exists between a person’s academic achievement and their intellectual ability (which may be very high).
People with dyslexia may have talents in many areas, in addition to their areas of difficulty. Each person’s pattern of strengths and weaknesses is unique to them. In other words, no two dyslexics are alike. That is why assessment is very important.
Common Signs of Dyslexia:
Early signs
- difficulty learning to talk
- difficulty listening and following directions
- difficulty remembering
- difficulty pronouncing words correctly or expressing ideas clearly
In school
- difficulty learning the alphabet
- difficulty sequencing letters or numbers
- difficulty rhyming
- difficulty with sequence and memory for words
- difficulty learning to read, write and spell
About Phonological Processing
Extensive studies have shown that children diagnosed with dyslexia consistency differ from other children in an ability called “phonological processing”. Phonological processing involves the ability to notice, think about, and manipulate the individual sounds in words (phonemes).
A phoneme is the smallest sound portion of a word, smaller than a syllable. Children have to be able to hear and distinguish phonemes in words before they can attach letters or letter combinations to them. Rhyming is an early activity encouraging the development of “phoneme” awareness.
Diagnosis & Treatment
Diagnosis of dyslexia is based on a comprehensive assessment that may include tests of: intellectual ability, expressive and receptive language (both oral and written), academic achievement in reading, spelling, vocabulary, comprehension, handwriting and composition. Recommendations for educational remediation should be contained in a written report.
Appropriate remedial programming for dyslexia may include the following:
- direct instruction of language skills and concepts.
- systematic, step-by-step sequential teaching of the alphabetic phonic system of language
- multisensory instruction, involving seeing, listening, touching and doing
Dyslexia is something that people are born with, and in many cases there appears to be a family history. Ongoing research is documenting differences in the structure and organization of the brains of people with dyslexia.
Dyslexia is not outgrown, but with appropriate education, understanding and time, many people with dyslexia learn to read and write, and go on to develop their special abilities and talents. They may be very successful in their chosen careers. A number of well-known scientists, artists, athletes and business and political leaders have dyslexia.
Learning Disabilities Association of Ontario
When a child is identified as having a learning disability, we know two things: he or she has at least average intelligence, and possibly above average; and he or she learns in a different way. This means that the child is what we call an “exceptional student,” and that the exceptionality is in the area of communications. This area covers the ability to process information. As simple as all this may sound, unlocking the mystery of how an individual child with a learning disability learns is a tremendous challenge. Think of the circuitry of a computer. As complex as it may be, all the bits and pieces are labeled and, if there is a malfunction, a trained technician can find the problem and fix it. The human brain, on the other hand, is infinitely more complex than a computer. Even the best neurosurgeons cannot repair the malfunctions in a person’s ability to process information.
Processing information appears to require skills in four basic areas:
- the reception of information;
- the integration or organization of that information;
- the ability to retrieve information from its storage in the brain; and
- the communication of retrieved information to others.
Difficulties in any of these areas can seriously affect a child’s ability to learn in a normal way, and these same difficulties may prevent the child from developing social competence or the ability to interact effectively with his or her peers or with adults. Each area of difficulty is composed of many skills, and many of the areas overlap with others or are dependent on others. Discovering the specifics of an individual child’s difficulties is a very complicated task. In addition, each child’s set of characteristics is unique. He or she may have difficulties in only one or two of the areas, or there may be difficulties in most of the areas. The severity of these difficulties ranges from mild, to moderate, to severe, thus adding a further set of complications.
Using formal and informal assessments, interviews, and observations, we attempt to piece together the puzzle. The most common characteristics, or “classic symptoms” are found in the following list of abilities:
- auditory perceptual skills: understanding what we hear;
- visual perceptual skills: understanding what we see;
- processing speed: the time it takes to process information;
- organization: keeping information in order in the right place;
- memory: short-term and long-term storage and retrieval of information;
- fine motor skills: legible and effective written communication including copying what is seen;
- gross motor skills: control of body parts in walking, working and playing;
- attention: focusing on one thing for the required length of time;
- abstractions: interpreting symbolism; and
- social competence: effective interactions with others.
The frustrations and anxieties that the child with a learning disability experiences are beyond the comprehension of those of us who learn and get along with others satisfactorily. The most devastating result for these children is the gradual deterioration of their self‑esteem, and everything must be done to help these children maintain it.
The common side effects of having a learning disability may include distractibility, impulsiveness, mood changes, inconsistencies, work‑avoidance behaviour, attention‑seeking behaviours, and oppositional behaviours. Often, these behaviours develop to mask the real problems that children with learning disabilities face on a daily basis. However, if we take the time to talk to them, they will say that they only want to learn and to have friends like everyone else. With the right support and an individualized learning program they can be successful!
Paul Thompson has been a Resource Services Consultant at Amethyst School in London, a Provincial Demonstration School for students with severe learning disabilities and a resource facilitator with the Learning Disabilities Association of London Region.
Reprinted with permission from OPSTF News
Author: Margaret Amerongen
Source: Among Friends – Integra’s Newsletter
In previous issues of Among Friends we noted that problems in behaviour and lifeskills associated with learning disabilities are mistakenly attributed to negative character traits such as laziness, stubbornness, and uncooperativeness. Grasping “the view from within” and putting ourselves in the shoes of children and youth with learning disabilities is critical in order to effectively understand and help them.
An increasing number of children and youth seeking Integra’s services have learning profiles with the constellation of traits called “nonverbal learning disability” (NLD). This is a complex disorder, often not well understood by caregivers and educators.
Children with NLD often have relatively well-developed vocabulary and rote memory for facts, but struggle in one or more of the following areas:
- visual-spatial skills: poor understanding of what is taken in visually, poor perception of the relative positions of objects in space
- organizational skills: how things fit together in patterns, in time, and in space; e.g. breaking tasks down into component parts and combining parts to make the whole
- motor skills: physical awkwardness, writing problems
- social and emotional problems due to difficulty processing complex or novel information. These children have trouble learning the meaning of the actions, the nonverbal behaviour, and the emotions of others. They struggle with adjusting to novelty or transitions. All of this leads to problems in social judgement and social interaction.
Children with NLD are often labeled as behaviour problems because it is not recognized that their problems are neurological in origin.
Everyday tasks can be confusing and overwhelming for children with NLD. These can include:
- finding their way around a school or a neighbourhood
- remembering where they put things or how to find them; tidying a room, notebook or knapsack
- coping with the complexity of a group of children playing: what is fair, what is socially acceptable to say or do, how to appropriately enter and continue a conversation
- adjusting to any alteration in routine or grasping a change in rules or method of completing tasks
Children with NLD often have “meltdowns” or detach themselves by “spacing out” because they are overloaded with the sheer effort of navigating situations that other children learn to cope with automatically.
For example, the child may avoid or react angrily to any sort of novelty because he or she is not able to quickly and accurately understand the new situation. Children with NLD often talk incessantly. This may be because they rely heavily on their well-developed language skills to interact with others and to cope with ever-present confusion and anxiety. Social problems frequently occur because the child with NLD does not understand the idea of “personal space”, or the nonverbal signals that other people use to convey irritation, anxiety, etc. Often the child does not understand the give and take of play and conversation. He or she may be unaware that the listener is bored. The child with NLD may try to control play in order to cope with his or her uncertainty and anxiety. The child with NLD frequently but unintentionally makes inappropriate comments and then is bewildered when others become upset.
What caregivers and teachers can do:
- Learn as much as they can about NLD and how it specifically affects their own child. This will help them to understand the meaning of the child’s behaviour and to set realistic expectations for him or her. This knowledge will help the caregiver to attain “the view from within” and put her or himself in the child’s shoes in order to compassionately and effectively help. Lack of knowledge about NLD can lead to unrealistic demands and expectations and frequent criticism. The heartbreaking result can be serious erosion in the child’s self esteem and in the caregiver’s self-confidence.
- Recognize that uncooperative behaviour may be the result of feeling confused, anxious and overwhelmed.
- Give the child verbal direction and instruction. Use the child’s verbal strengths to help him learn from explicit instruction what other children learn implicitly. Explicitly teach him or her such details as: what is expected in different social, family, and school situations; how others feel, how to organize and carry out tasks, etc. It has been wryly noted (see Sue Thompson’s book below) that parents may find themselves saying of their child with NLD, “I shouldn’t have to tell you everything!”. The truth is that the child with NLD does need to be taught a lot of what other children learn automatically – they need to be taught, however, with kindness and patience.
- Manage the environment. Children with NLD need predictable schedules as much as possible. They need preparation for changes in routines and to be given notice that they are about to be asked to make a transition in activities. They need advance planning and instruction about unfamiliar tasks and situations.
This article can provide only the briefest of introductions to NLD and suggestions for coping. Our information is drawn from the following books:
Nonverbal Learning Disorders at Home by Pamela Tanguay
The Source for Nonverbal Learning Disorders by Sue Thompson
Helping a Child with Nonverbal Learning Disorder or Asperger’s Syndrome by Kathryn Stewart
All of these books are available at local bookstores.
Reprinted with permission from Integra, Among Friends, Fall/Winter 2002, www.integra.ca
Auditory Processing Deficits and Central Auditory Processing Disorders (C.A.P.D.)
Learning disabilities are related to the inadequate development of a number of processing areas. Visual perceptual deficits have been a concern of educators over the years and there is a growing recognition that good auditory processing abilities are essential for successful academic progress and they can influence classroom behaviour.
Auditory acuity is the ability to detect the presence of sounds at various levels of intensity and frequency. It’s only one of many auditory abilities, yet it’s the only competency many teachers consider when evaluating a child’s listening skills.
Other auditory abilities are not as widely understood and not as easily addressed.
Auditory attention is the ability to direct and sustain attention to preferred sound messages. Those with auditory attention problems have difficulty selecting relevant from irrelevant sounds (poor auditory figure-ground ability).
Auditory memory is the ability to remember auditory sound patterns. Children build a reserve of previously learned sound patterns from which they recall and then interpret and integrate their auditory environment.
Auditory discrimination is the ability to detect similarities and differences between sounds. Those with poor discrimination may not, for example, be able to hear the difference between the words took and book.
Auditory synthesis (integration) is the ability to blend independent sound units into complete aural units (words) such as c-ar-t, or t-a-ble.
Auditory comprehension is the ability to decode and derive meaning from sound messages. This requires competence in several auditory abilities: attention, memory, discrimination and integration.
Auditory-visual integration is the ability to integrate auditory and visual messages. Because sound is fleeting, visual stimuli often support the interpretation of sound. Associating a picture or the printed word with the spoken word is an auditory-visual integration activity.
Children who have auditory processing deficits often find reading, writing and spelling difficult because these skills require an ability to: recognize and distinguish between sounds in words; blend them together; separate words into syllables; and, follow auditory sequences. Many children with Central Auditory Processing Disorder (CAPD) also have speech and language deficits such as low vocabulary, poor flexibility of vocal patterns and articulation problems.
Evaluation by both an audiologist and a speech-language pathologist provides important information about the child with central auditory processing problems. An audiologist who is experienced with CAPD can evaluate a child’s hearing and do further testing for possible auditory processing problems. A speech-language pathologist can evaluate a child’s perception of speech and his/her receptive (understanding) and expressive (production) language use. These professionals and a child’s teacher and parents can work together to determine the scope of the problem and the most effective treatment techniques.
All auditory abilities are interrelated – each one influencing the other. However certain situations can place greater demands on any one of these abilities. In recent years, the regular classroom has become a very busy, very noisy environment. Desks are clustered together in order to facilitate interactive learning activities. The burden of this classroom configuration on sensitive listeners is the likely reason more children with C.A.P.D. are coming to the attention of the professionals.
Many children with C.A.P.D. exhibit behaviour similar to children with ADHD. They may also: speak too loudly; appear to daydream; get lost in rote verbalizations; not enjoy music; avoid explanations by using phrases like, “I forget.”; substitute gestures for words; lip read; have trouble with phonics-based activities; and look to see what others are doing before beginning an activity.
Some assistive devices, like amplified sound and noise cancellation systems, are now being developed to aid sensitive listeners. Teacher awareness of auditorally sensitive students is crucial.
Auditory processing deficits may be part of learning disabilities, but a diagnosis of CAPD by an audiologist is not sufficient to diagnose learning disabilities, which are diagnosed by psychology professionals.
Author: Kate Lloyd and Jeff Clayton
Source: LDAO
1. Myth: Learning disabilities (LDs) do not really exist.
Fact: LDs are real. Recent research indicates neurological differences in the brain structure and function for people who have learning disabilities.
2. Myth: Learning disabilities are all the same and/or easily understood.
Fact: Learning disabilities are complicated. The extent of their impact and the areas of learning they affect vary greatly from person to person; combine in any variety of ways; and vary depending on context.
Helping is not as complicated: people with LDs need to determine which modes of learning work well for them, and use these strengths to compensate for the areas affected by their LD.
3. Myth: Students with LDs cannot learn.
Fact: Students with LDs can be successful learners, at all levels and in any situation, by compensating for their weaknesses by using their strengths; by using alternative, individualized teaching and learning materials and methods; and by choosing tasks that suit themselves.
4. Myth: More boys than girls have learning disabilities.
Fact: Although four times as many boys as girls are identified as having LDs by schools, research studies suggest that many girls who are not identified also have the most common form of learning problem – difficulty with reading. Many girls’ learning difficulties are neither identified nor treated – possibly because boys who are struggling are, in general, more disruptive in classes.
5. Myth: Students with LDs are just lazy.
Fact: Students with LDs generally have to spend more time to adequately complete school assignments. This extended effort can often lead to difficulties in completing assignments on time, maintaining course requirements such as tutorial reading and studying. These difficulties should not be misinterpreted as ‘laziness’.
6. Myth: Students diagnosed with LDs at school age should have outgrown them by adulthood.
Fact: LDs are a lifelong condition. If the diagnosis of a learning disability in childhood is accurate, the disability will endure into adulthood. Specific learning strategies and adjustments can be developed to address problems, and can make it so that LDs are not a pressing issue, but the learning disability itself remains.
7. Myth: Learning disabilities are a school issue.
Fact: LDs affect one or more modes of learning, anywhere that mode is used. LDs tend to be noticed most often when they impact on school-learning, but exist in all areas of life – work, family, relationships, etc.
8. Myth: Accommodating the needs of students with LDs in schools is too difficult, time consuming and expensive.
Fact: Accommodations implemented for students with LDs are also generally good examples of universal learning strategies. They can improve teaching and learning, not just for students with LDs, but also for the overall student population and other minority groups, such as people from a non-English speaking background. Teachers can also benefit from this approach by developing a range of flexible teaching and learning strategies that can be implemented in a number of different environments.
9. Myth: Providing academic adjustments such as accommodations and individualized teaching gives students with LDs an unfair advantage over other students.
Fact: Academic adjustments are determined on identified deficit’s resulting from a student’s LDs. Adjustments ensure equal and fair participation in a learning environment and ensure actual learning is recognized. Students with LDs are required to meet the same academic standards as their peers.
10. Myth: LDs can be cured.
Fact: There have been occasional claims by individuals of “curing” learning disabilities in various ways. Learning disabilities are a life-long condition; many people learn to successfully cope with their LDs to such an extent that it is no longer an issue for them, and certain intensive study methods do help some people, but there is no researched evidence that one person’s solution will work for all.
Author: Coordinated Campaign for Learning Disabilities.
Source: Reprinted with permission of the Coordinated Campaign for Learning Disabilities.
The good news about learning disabilities is that scientists are learning more every day. Their research provides hope and direction.
If parents, teachers, and other professionals discover a child’s learning disability early and provide the right kind of help, it can give the child a chance to develop skills needed to lead a successful and productive life. A recent National Institutes of Health study showed that 67% of young students who were at risk for reading difficulties became average or above average readers after receiving help in the early grades.
Parents are often the first to notice that “something doesn’t seem right.” If you are aware of the common signs of learning disabilities, you will be able to recognize potential problems early. The following is a checklist of characteristics that may point to a learning disability. Most people will, from time to time, see one or more of these warning signs in their children. This is normal. If, however, you see several of these characteristics over a long period of time, consider the possibility of a learning disability.
Preschool
- Speaks later than most children
- Pronunciation problems
- Slow vocabulary growth, often unable to find the right word
- Difficulty rhyming words
- Trouble learning numbers, alphabet, days of the week, colors, shapes
- Extremely restless and easily distracted
- Trouble interacting with peers
- Difficulty following directions or routines
- Fine motor skills slow to develop
Grades K-4
- Slow to learn the connection between letters and sounds
- Confuses basic words (run, eat, want)
- Makes consistent reading and spelling errors including letter reversals (b/d), inversions (m/w), transpositions (felt/left), and substitutions (house/home)
- Transposes number sequences and confuses arithmetic signs (+, -, x, /, =)
- Slow to remember facts
- Slow to learn new skills, relies heavily on memorization
- Impulsive, difficulty planning
- Unstable pencil grip
- Trouble learning about time
- Poor coordination, unaware of physical surroundings, prone to accidents
Grades 5-8
- Reverses letter sequences (soiled/solid, left/felt)
- Slow to learn prefixes, suffixes, root words, and other spelling strategies
- Avoids reading aloud
- Trouble with word problems
- Difficulty with handwriting
- Awkward, fist-like, or tight pencil grip
- Avoids writing compositions
- Slow or poor recall of facts
- Difficulty making friends
- Trouble understanding body language and facial expressions
High School Students and Adults
- Continues to spell incorrectly, frequently spells the same word differently in a single piece of writing
- Avoids reading and writing tasks
- Trouble summarizing
- Trouble with open-ended questions on tests
- Weak memory skills
- Difficulty adjusting to new settings
- Works slowly
- Poor grasp of abstract concepts
- Either pays too little attention to details or focuses on them too much
- Misreads information
Nonverbal Learning Disability describes a well-defined profile that includes strengths in verbal abilities contrasted with deficits in visual-spatial abilities.
Individuals with NVLD often have trouble with some of the following: organization, attention, executive functioning, nonverbal communication, and motor skills.
NVLD Characteristics
A significant discrepancy between verbal comprehension and perceptual reasoning abilities, in which verbal skills are greater than perceptual skills, is a necessary feature to make the NVLD diagnosis, but it is not sufficient in the absence of sustained academic, professional, social, and emotional difficulties.
Relative Verbal Strengths and Perceptual Deficits
Children with NVLD have strengths in verbal reasoning, such as a well-developed vocabulary, rote learning skills, strong factual recall when information is presented without context, and remembering concrete details from a story. In contrast, they have trouble understanding the “big picture” and identifying the main idea in a narrative. Children with NVLD also struggle with life skills that require an understanding of spatial relationships, such as recognizing how parts fit together into a whole, completing jigsaw puzzles and building with blocks, learning routes for travel, and manipulating objects in space.
Fine Motor Control Deficits
Children with NVLD have trouble developing fine-motor skills and may have poor handwriting, difficulty learning to tie their shoelaces, and problems using small tools and utensils.
Executive Functioning and Attention Deficits
Children with NVLD may have weak executive functions or difficulty sustaining their attention. However, whether these problems are essential attributes of NVLD, or are simply common co-occurring issues in children who come to clinical attention, is unknown. These children may have trouble handling new tasks, solving problems and remaining flexible in their thinking. They may also have difficulty staying focused, completing multi-step instructions, organizing tasks and materials, controlling their impulses, and they may have other symptoms associated with Attention-Deficit/Hyperactivity Disorder (ADHD).
Social Difficulties
Children with NVLD are usually interested in social relationships and have the capacity for empathy, but may report feeling isolated and complain that they do not have satisfying relationships with their peers. Children with NVLD can have trouble understanding humor, which may contribute to their social problems. Clinicians believe that children with NVLD may suffer from depression and anxiety disorders more than children without NVLD, although this clinical impression currently lacks strong empirical support. A significant discrepancy between verbal comprehension and perceptual reasoning abilities, in which verbal skills are greater than perceptual skills, is a necessary feature to make the NVLD diagnosis.
Academic Difficulties
Children with NVLD may have difficulty learning math concepts and procedures. In early years of school they may have trouble with numerocity, telling time, the value of coins, and greater-than and less-than relationships. In later years they may have problems translating fractions to decimals and associated procedures. Identifying and describing geometric shapes and reading graphs and charts may be difficult for children with NVLD. Children with NVLD may have trouble with certain language-based tasks in school that require understanding the big picture or solving new problems. For example, beginning in 3rd or 4th grade, they may have trouble with reading comprehension, as opposed to in earlier years when the focus was on sounding out words and the structure of stories. Children with NVLD may have a hard time answering inferential questions about literature. They also may have problems interpreting metaphors and understanding multiple meanings of words in a text. For similar reasons, they may have difficulty writing essays and trouble identifying information and evidence that support their point of view or thesis.
Excerpted from https://nvld.org/for-clinicians-and-scientists/
The NVLD Project is dedicated to raising awareness, building support, and creating helpful solutions for children, adolescents, and adults with Non-Verbal Learning Disability. This goal is accomplished through a variety of programs, including educational workshops, research, and community outreach. Long term, The NVLD Project seeks to define and establish NVLD as a valid disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM).